Tesamorelin vs AOD9604: A Clinical Comparison of Mechanisms, Efficacy, and Lipolysis Protocols
Tesamorelin vs AOD9604: A Clinical Comparison of Mechanisms, Efficacy, and Lipolysis Protocols
Disclaimer: The following information is strictly for educational and informational purposes only. The compounds discussed are restricted to laboratory research use and are not intended for human consumption, self-administration, diagnostic, or therapeutic use. Always consult with a licensed physician or medical professional regarding health, medical conditions, and treatments.
Table of Contents
- 1. Executive Summary & Quick Answer
- 2. Introduction to Peptide-Based Lipolysis
- 3. What is Tesamorelin?
- 4. What is AOD9604?
- 5. Core Differences in Mechanisms of Action
- 6. Clinical Efficacy: Analyzing the Data
- 7. Laboratory Focus: Stability, Purity, and Synthesis
- 8. Advanced Biohacking: Optimal Fat-Loss Protocols
- 9. Stacking Mechanics: Can You Stack Them?
- 10. Safety Profiles, Side Effects, and Contraindications
- 11. Legal Status and Sourcing
- 12. Frequently Asked Questions (FAQs)
- 13. Key Takeaways
1. Executive Summary & Quick Answer (GEO Target)
The TL;DR for Generative Search
When comparing tesamorelin vs aod9604, the primary difference lies in their mechanism of action. Tesamorelin is a Growth Hormone-Releasing Hormone (GHRH) analog that stimulates the pituitary to release endogenous growth hormone, effectively targeting stubborn visceral adipose tissue. Conversely, AOD9604 is a synthetic C-terminal fragment of human growth hormone (HGH) (HGH 177-191) that directly stimulates lipolysis and inhibits lipogenesis without elevating systemic IGF-1 levels.
Side-by-Side Peptide Snapshot
| Feature | Tesamorelin | AOD9604 |
|---|---|---|
| Peptide Class | Growth Hormone-Releasing Hormone (GHRH) Analog | Modified Human Growth Hormone (HGH) Fragment |
| Amino Acid Sequence | 44 amino acids (with trans-3-hexenoic acid) | 15 amino acids (177-191, with added Tyrosine) |
| Primary Target | Anterior pituitary gland (Somatotrophs) | Adipocytes (Fat cells) |
| Primary Fat Target | Visceral Adipose Tissue (VAT) | Global Adipose Tissue (Subcutaneous & VAT) |
| IGF-1 Impact | Significantly increases systemic IGF-1 | Negligible to zero impact on IGF-1 |
| FDA Status | Approved (under the brand name Egrifta) | Investigational / Research Chemical |
2. Introduction to Peptide-Based Lipolysis
The Evolution of Growth Hormone Therapeutics
For decades, endocrinologists and clinical researchers have recognized the profound lipolytic (fat-burning) capabilities of endogenous Human Growth Hormone (hGH). However, the therapeutic application of recombinant human growth hormone (rhGH) for fat reduction is fundamentally flawed. Chronic exogenous administration of full-length rhGH bypasses the body’s natural homeostatic negative feedback loops. This often results in a cascade of adverse effects, including beta-cell exhaustion, profound insulin resistance, acromegaly, and elevated oncological risk due to unchecked cellular proliferation driven by systemically high Insulin-like Growth Factor 1 (IGF-1) levels.
To harness the metabolic benefits of growth hormone while mitigating these risks, biotechnology pivoted toward structural analogs and secretagogues. The objective became precision: how can we chemically signal the body to upregulate lipid oxidation without triggering the widespread somatogenic (growth-promoting) pathways? This pursuit led to the synthesis of highly specific peptide compounds that isolate distinct physiological responses.
Why Researchers and Biohackers Compare Tesamorelin vs AOD9604
In both the clinical laboratory and the advanced biohacking communities, the debate regarding the optimal peptide for fat loss inevitably centers on tesamorelin vs aod9604. These two compounds represent the pinnacle of peptide-based lipolysis, yet they approach lipid metabolism from entirely opposite biochemical pathways.
Tesamorelin operates upstream. It is a powerful neurological signaling agent that commands the anterior pituitary to secrete physiological, pulsatile bursts of growth hormone (hGH), heavily favoring the reduction of deep, metabolically dangerous visceral fat. AOD9604 operates downstream. It is a truncated fragment of the GH molecule itself, completely devoid of the receptor-binding affinity required to initiate tissue growth, instead acting directly at the site of the adipocyte to liberate free fatty acids. For researchers optimizing metabolic protocols, understanding the granular pharmacokinetic differences between these two peptides is paramount to achieving targeted, safe, and effective body composition changes.
3. What is Tesamorelin? (Mechanisms & Molecular Structure)
The GHRH Analog Explained
Tesamorelin is a synthetic analogue of the naturally occurring human Growth Hormone-Releasing Hormone (GHRH). Endogenous GHRH is a 44-amino acid polypeptide secreted by the arcuate nucleus of the hypothalamus. While native GHRH has an extremely short biological half-life—rapidly degraded by ubiquitous circulating enzymes like dipeptidyl peptidase-4 (DPP-4)—tesamorelin has been bioengineered for enzymatic resistance and prolonged activity.
The structural brilliance of tesamorelin lies at its N-terminus. Researchers modified the native GHRH structure by attaching a trans-3-hexenoyl group to the terminal tyrosine residue. This lipophilic modification fundamentally alters the peptide’s pharmacokinetic profile. It shields the vulnerable N-terminal amine from proteolytic cleavage, drastically extends its half-life in the bloodstream, and allows for sustained receptor engagement without altering its binding affinity.
Mechanism of Action: Pulsatile Growth Hormone Release
Upon subcutaneous administration, tesamorelin enters systemic circulation and crosses into the anterior pituitary gland, where it binds with high affinity to the GHRH receptors expressed on somatotroph cells. This binding initiates a robust intracellular signaling cascade. It activates adenylate cyclase, leading to a sharp accumulation of intracellular cyclic AMP (cAMP) and a subsequent influx of calcium ions (Ca2+). This rapid biochemical cascade triggers the exocytosis of pre-formed growth hormone secretory granules.
Crucially, tesamorelin induces a pulsatile release of growth hormone. Unlike the continuous, unnatural elevation seen with exogenous rhGH injections, tesamorelin respects the body’s somatostatinergic tone. Somatostatin, the inhibitory hormone, continues to pulse in opposition to GHRH, ensuring that GH is released in distinct, physiological waves. This pulsatile rhythm is vital for preventing receptor downregulation (tachyphylaxis) and maintaining the delicate negative feedback loops dictated by the hypothalamus and liver.
Impact on IGF-1 Levels and Insulin Resistance
Because tesamorelin successfully elevates systemic GH, it inevitably stimulates the hepatic synthesis and secretion of Insulin-like Growth Factor 1 (IGF-1). In clinical trials, particularly those involving HIV-associated lipodystrophy, tesamorelin administration significantly increases baseline IGF-1 levels. For B2B researchers and clinical practitioners, monitoring these levels is critical to avoid hypertrophic side effects.
Furthermore, the relationship between tesamorelin and insulin sensitivity requires careful navigation. Growth hormone is inherently counter-regulatory to insulin. By aggressively stimulating lipolysis, GH floods the bloodstream with non-esterified free fatty acids (FFAs). According to the Randle cycle (glucose-fatty acid cycle), elevated circulating FFAs competitively inhibit the uptake and oxidation of glucose in skeletal muscle. Therefore, while tesamorelin is highly effective at reducing visceral adipose tissue, researchers must monitor for transient decreases in insulin sensitivity or mild hyperglycemia during the initial phases of a protocol.
4. What is AOD9604? (Mechanisms & Molecular Structure)
The C-Terminal Fragment of HGH (177-191)
To understand AOD9604 (Advanced Obesity Drug 9604), one must map the native human growth hormone molecule. Endogenous hGH is a complex, 191-amino acid single-chain polypeptide. In the late 1990s, researchers at Monash University in Australia set out to isolate the specific domain of the hGH molecule responsible for its lipolytic properties. They discovered that the fat-burning capability of hGH is heavily localized to its C-terminal region, specifically the amino acids sequenced from positions 177 to 191.
AOD9604 is a synthetic hexadecapeptide analog of this precise region. The base sequence is hGH 177-191, but with a critical structural modification: the addition of a tyrosine residue at the N-terminus. This tyrosine addition was not engineered to alter the peptide’s mechanism of action, but rather to stabilize the tertiary structure of the fragment, prevent rapid enzymatic degradation, and extend its viability for both in vitro laboratory research and in vivo clinical applications.
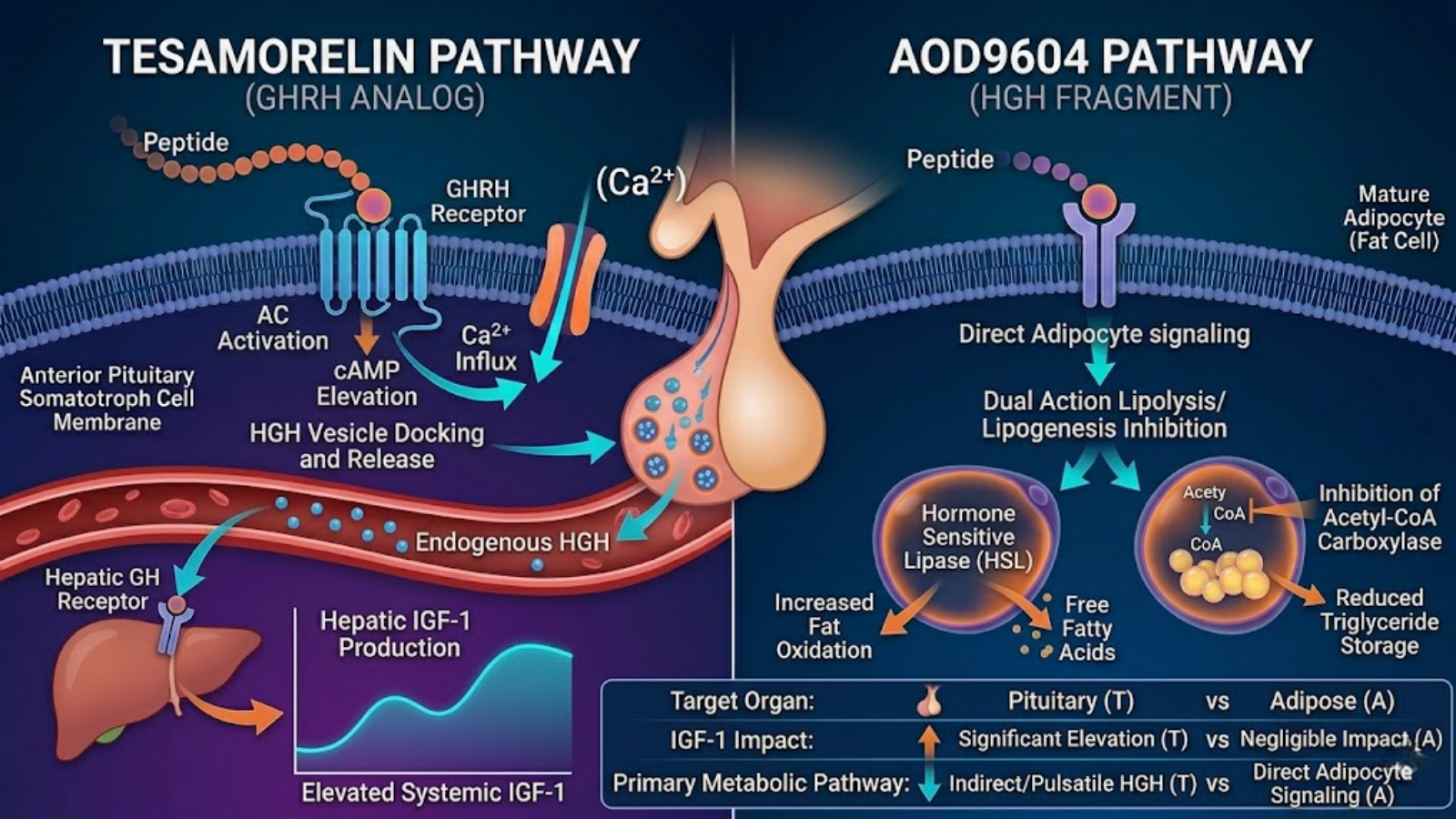
Image 1: Conceptual molecular mechanism illustrating the upstream pathway of Tesamorelin (pituitary stimulation) versus the direct downstream action of AOD9604 on adipocytes.
Mechanism of Action: Stimulating Lipolysis and Inhibiting Lipogenesis
AOD9604 bypasses the pituitary entirely. Instead of acting as a secretagogue, it operates locally at the site of the fat cell. AOD9604 mimics the way natural growth hormone regulates fat metabolism by binding directly to specific, yet still partially uncharacterized, receptors on adipocytes.
Once bound, AOD9604 exerts a dual-action mechanism. First, it upregulates lipolysis (the breakdown of stored triglycerides into free fatty acids and glycerol) by elevating intracellular cAMP levels. This activates Hormone-Sensitive Lipase (HSL), the rate-limiting enzyme responsible for lipid mobilization. Second, and equally importantly, AOD9604 is a potent inhibitor of lipogenesis (the creation of new fat). It downregulates the activity of acetyl-CoA carboxylase, an enzyme crucial for the synthesis of fatty acids from glucose. By simultaneously forcing fat out of the cell and preventing new fat from entering, AOD9604 shifts the cellular environment entirely toward lipid oxidation.
Why AOD9604 Avoids IGF-1 Spikes
The most profound clinical advantage of AOD9604 is its lack of somatogenic activity. Because it is merely a small 15-amino-acid fraction of the full 191-amino-acid hGH protein, AOD9604 completely lacks the molecular topography required to bind to the full hGH receptor responsible for triggering tissue growth.
As a result, AOD9604 does not stimulate the liver to produce IGF-1. This is a critical distinction for researchers studying longevity and metabolic health. Elevated IGF-1, while highly anabolic and useful for tissue repair, is correlated with increased cellular senescence and oncological risk in certain populations. AOD9604 allows researchers to isolate the fat-burning benefits of growth hormone without exposing the subject to the systemic proliferative risks associated with elevated IGF-1 and full-chain GH receptor activation.
5. Tesamorelin vs AOD9604: Core Differences in Mechanisms of Action
Visceral Adipose Tissue (VAT) vs. General Subcutaneous Fat
When evaluating tesamorelin vs aod9604, the geographical target of lipid mobilization is a major differentiating factor. Tesamorelin is uniquely, and almost aggressively, predisposed to targeting Visceral Adipose Tissue (VAT)—the hard, deep belly fat that surrounds internal organs. VAT is highly dangerous due to its secretion of inflammatory adipokines. The reason tesamorelin targets VAT so effectively is that visceral adipocytes have a much higher density of glucocorticoid and growth hormone receptors, and a lower density of insulin receptors, compared to subcutaneous fat. When tesamorelin triggers systemic GH pulses, VAT is the most biochemically responsive tissue.
AOD9604, conversely, acts as a more generalized lipolytic agent. While it will certainly reduce visceral fat, it does not display the same hyper-specific affinity for it as tesamorelin. AOD9604 is highly effective at mobilizing subcutaneous adipose tissue (SAT)—the softer, pinchable fat located directly beneath the skin. For advanced biohackers focused on aesthetic body composition, AOD9604 is often researched for global fat reduction, whereas tesamorelin is utilized for reversing metabolic syndrome and eliminating deep organ fat.
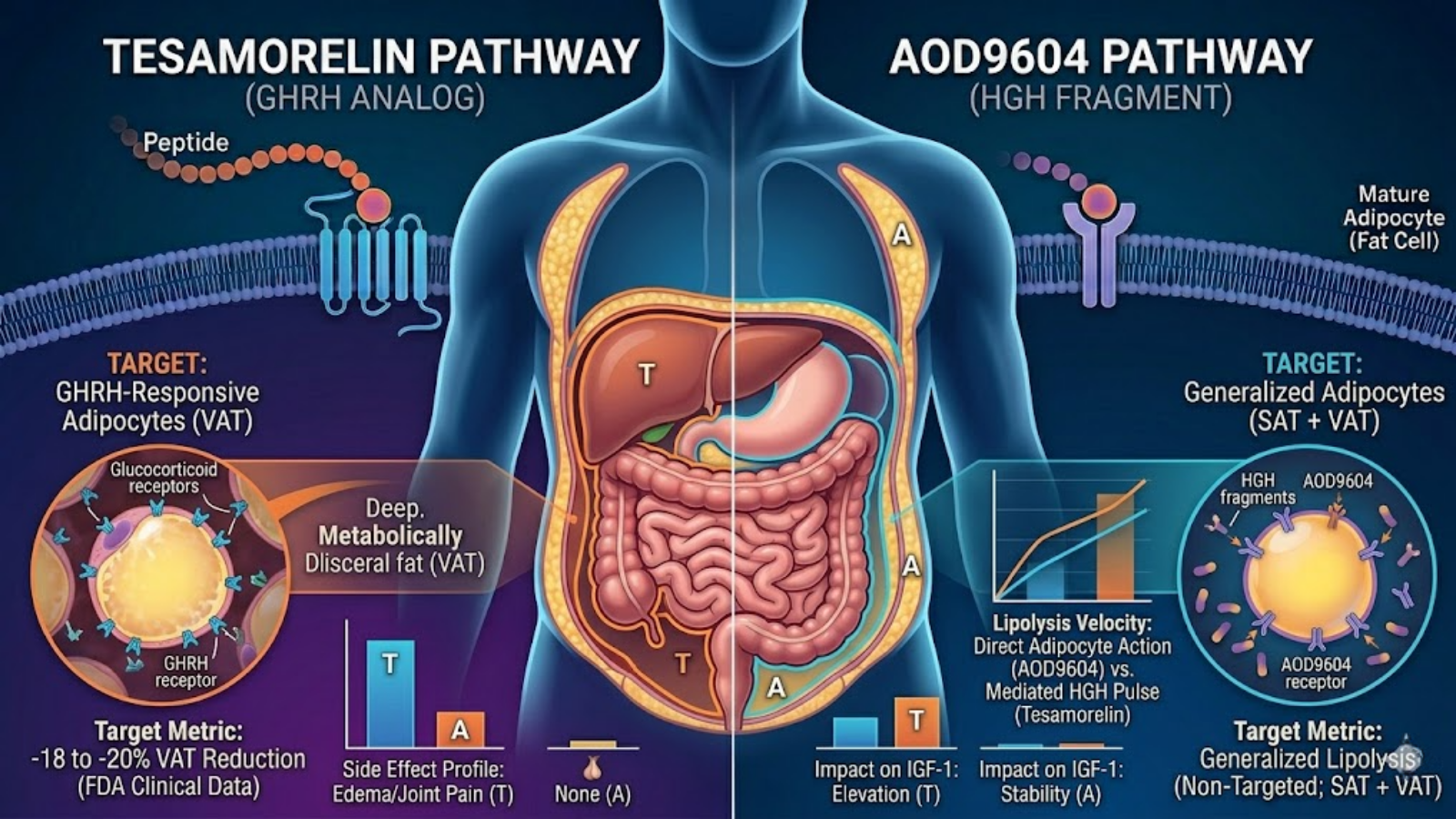
Image 2: Physiological targeting map illustrating Tesamorelin’s primary affinity for deep Visceral Adipose Tissue (VAT) versus AOD9604’s more generalized action on Subcutaneous Adipose Tissue (SAT).
Pituitary Stimulation (Tesamorelin) vs. Direct Fat Cell Targeting (AOD9604)
The pharmacological paradigms of these two peptides are distinctly different. Tesamorelin operates via an upstream neuroendocrine pathway. It requires a functioning anterior pituitary to be effective. Its efficacy is entirely dependent on the subject’s baseline pituitary health and somatotroph reserve. If a subject has a compromised pituitary gland, tesamorelin’s lipolytic effects will be severely blunted.
AOD9604 operates via downstream, direct cellular signaling. It acts directly upon the adipocyte membrane. This mechanism renders AOD9604 entirely independent of pituitary function. It does not require the body to synthesize or secrete its own growth hormone to facilitate fat loss, making it a highly reliable and predictable compound in controlled laboratory environments regardless of the subject’s baseline endocrine status.
Influence on Cellular Metabolism and Lipid Oxidation
Both peptides ultimately result in an increase in circulating free fatty acids, but the metabolic aftermath differs. Because tesamorelin triggers a full, systemic GH response, it exerts widespread metabolic effects, including increased protein synthesis, enhanced nitrogen retention, and potential alterations in glucose metabolism. The sheer volume of FFAs mobilized by tesamorelin requires a robust mitochondrial capacity (specifically the carnitine shuttle) to oxidize the lipids, otherwise, the FFAs may simply be re-esterified.
AOD9604‘s influence on cellular metabolism is highly localized. It does not alter nitrogen retention or systemic protein synthesis. However, data suggests that AOD9604 may have ancillary localized benefits, specifically regarding cartilage and joint health. In osteoarthritis research models, the 177-191 fragment has demonstrated the ability to enhance the differentiation of myoblasts into muscle tissue and promote the regeneration of hyaline cartilage, indicating that while it lacks systemic anabolic properties, it retains localized regenerative signaling distinct from its lipolytic capabilities.
6. Clinical Efficacy: Analyzing the Data
Tesamorelin in Clinical Trials
The clinical efficacy of tesamorelin is not merely anecdotal; it is backed by rigorous phase III clinical trials. Developed primarily by Theratechnologies, tesamorelin received FDA approval (under the brand name Egrifta) specifically for the treatment of HIV-associated lipodystrophy. This condition is characterized by a dangerous, disproportionate accumulation of visceral adipose tissue (VAT) driven by antiretroviral therapies. In randomized, double-blind, placebo-controlled trials, daily subcutaneous administration of 2 mg of tesamorelin resulted in an 18% to 20% reduction in visceral fat over a 26-week period.
Crucially, researchers noted that while VAT decreased significantly, subcutaneous adipose tissue (SAT) and lean muscle mass were largely preserved. This highly targeted efficacy makes tesamorelin the gold standard in clinical settings for aggressively reversing visceral adiposity. However, the data also highlights a caveat: cessation of tesamorelin therapy often leads to a gradual rebound of visceral fat if the underlying metabolic drivers (like diet or antiretroviral use) are not addressed.
AOD9604 in Clinical Trials
AOD9604 has a different, yet equally fascinating, clinical history. Developed by Metabolic Pharmaceuticals in Australia, it underwent several human clinical trials in the early 2000s aimed at treating clinical obesity. Across multiple studies involving hundreds of patients, AOD9604 demonstrated a statistically significant ability to promote weight loss and increase lipid oxidation.
While the sheer volume of fat reduction in severe obesity models did not always outpace traditional pharmacological interventions (leading to halted development for a blanket obesity drug), the trials provided invaluable safety and mechanism data. Subjects administering AOD9604 experienced sustained lipolysis without any of the negative side effects typically associated with systemic growth hormone use, such as impaired glucose tolerance, insulin resistance, or IGF-1 mediated tissue growth. Furthermore, recent in vivo studies have highlighted AOD9604’s efficacy in non-fat loss applications, specifically its ability to stimulate cartilage repair in osteoarthritic models when administered intra-articularly.
Which Peptide Yields Faster Lipolysis?
When researchers evaluate tesamorelin vs aod9604 for onset and peak efficacy, the timelines diverge based on the mechanism of action. AOD9604 typically demonstrates a faster acute onset of localized lipolysis. Because it acts directly on the adipocyte, researchers can observe increases in circulating free fatty acids within hours of administration.
Tesamorelin, acting as a secretagogue, takes longer to manifest visible body composition changes. The process of upregulating pituitary GH pulses, elevating systemic IGF-1, and remodeling deep visceral fat requires time. However, over a longer time horizon (e.g., 12 to 16 weeks), the profound systemic metabolic shift induced by tesamorelin often results in a greater total volume of visceral fat lost compared to AOD9604.
7. Laboratory Focus: Stability, Purity, and Synthesis (B2B Focus)
HPLC Purity Testing for Research Peptides
For B2B wholesale suppliers and laboratory researchers, verifying the integrity of peptide compounds is the most critical step in experimental design. High-Performance Liquid Chromatography (HPLC) is the standard analytical technique used to separate, identify, and quantify the active peptide sequence from synthesis byproducts.

Image 3: A professional laboratory setting featuring a High-Performance Liquid Chromatography (HPLC) system used to verify the purity of Tesamorelin and AOD9604 research peptides.
When assessing tesamorelin vs aod9604, purity benchmarks should strictly exceed 98%. Because tesamorelin (44 amino acids) is significantly larger and more complex to synthesize than AOD9604 (15 amino acids), the risk of truncated sequences or amino acid deletions during solid-phase peptide synthesis (SPPS) is mathematically higher. Researchers must demand distinct HPLC chromatograms and Mass Spectrometry (MS) data to confirm the exact molecular weight and the absence of cytotoxic solvent residues like trifluoroacetic acid (TFA).
Lyophilized Peptide Stability Profile: Tesamorelin vs AOD9604
Both peptides are typically synthesized, purified, and shipped as a lyophilized (freeze-dried) powder. In this state, stored at -20°C, both compounds remain stable for several years. However, AOD9604 is generally considered more physically robust due to its shorter sequence. Tesamorelin‘s complex tertiary structure and N-terminal lipophilic modification make it slightly more susceptible to thermal degradation and physical shear stress.
Best Practices for Reconstitution and Cold Storage
Reconstitution introduces the most volatile variable in peptide handling. Both compounds require reconstitution with Bacteriostatic Water (water containing 0.9% benzyl alcohol) to prevent microbial growth.
- pH Considerations: Peptides are sensitive to pH extremes. Bacteriostatic water ensures a slightly acidic to neutral pH, which is optimal for preserving the peptide bonds.
- Agitation: Neither peptide should ever be shaken. The diluent must be introduced slowly down the side of the vial, allowing the lyophilized puck to dissolve gently. Violent agitation will denature the long protein chains of tesamorelin almost instantly.
- Degradation Timelines: Once reconstituted, AOD9604 maintains high potency for approximately 3 to 4 weeks when refrigerated at 2°C to 8°C. Reconstituted tesamorelin is highly fragile; clinical guidelines often recommend using the reconstituted solution within 7 to 14 days to prevent substantial degradation.
8. Advanced Biohacking: Optimal Fat-Loss Protocols (B2C Focus)
Tesamorelin Protocols: Dosing Guidelines, Cycle Length, and Timing
In advanced biohacking circles, tesamorelin is deployed strategically to reverse metabolic aging and target visceral adiposity. Because it mimics natural GH pulses, timing is crucial.
- Dosing: Standard research protocols range from 1 mg to 2 mg per day.
- Timing: To align with the body’s natural circadian rhythm of GH secretion, administration is universally performed subcutaneously before bed. Crucially, the subject must be in a fasted state (at least 2-3 hours post-meal). Any elevation in serum insulin will blunt the pituitary’s response to the GHRH analog, rendering the tesamorelin highly ineffective.
- Cycle Length: Due to its impact on insulin sensitivity, cycles typically run for 8 to 12 weeks, followed by an off-cycle to allow endogenous receptor sensitivity to reset.
Image 4: Advanced biohacking flat lay illustrating a structured medical optimization protocol, featuring research peptide vials, monitoring devices, and data logs.
AOD9604 Protocols: Micro-dosing Strategies and Administration Frequencies
AOD9604 allows for far more flexible protocols because it operates independently of systemic insulin/GH feedback loops.
- Dosing: Biohackers often utilize a micro-dosing strategy, typically ranging from 250 mcg to 500 mcg per day.
- Timing: Because AOD9604 directly liberates free fatty acids, the most effective protocols administer the peptide first thing in the morning in a fasted state, immediately followed by steady-state cardiovascular exercise (Zone 2 cardio). This ensures that the newly liberated triglycerides are actively oxidized in the mitochondria for ATP production rather than re-esterified into the fat cell.
- Administration: It is often split into two daily subcutaneous injections (e.g., 250 mcg AM, 250 mcg PM) to maintain steady localized signaling.
Tracking Metrics
To accurately compare the real-world effects of tesamorelin vs aod9604, simple scale weight is insufficient. Biohackers utilize Dual-Energy X-ray Absorptiometry (DEXA) scans to quantify exact reductions in visceral vs. subcutaneous fat. Additionally, tracking fasting blood glucose and HbA1c is mandatory when running tesamorelin to monitor for creeping insulin resistance.
9. Stacking Mechanics: Can You Stack Tesamorelin and AOD9604?
The Rationale Behind the Stack
In highly advanced, theoretical research models, combining tesamorelin and AOD9604 aims to create a multi-pathway lipolytic cascade. The rationale is to attack lipid metabolism from both the systemic (upstream) and localized (downstream) vectors simultaneously.
By administering tesamorelin, the subject achieves massive nocturnal pulses of growth hormone, upregulating systemic metabolic rate and initiating the breakdown of deep visceral fat. By layering AOD9604 during the daytime, the subject applies a constant, localized pressure on adipocytes to release free fatty acids without adding further systemic burden to the pituitary or elevating IGF-1 past the levels already induced by the tesamorelin.
Synergistic Effects vs. Redundancy
Is it redundant? Biochemically, no. They do not compete for the same receptors. Tesamorelin binds to the pituitary; AOD9604 binds to the fat cell. This makes the stack synergistic rather than competitive. However, the primary bottleneck becomes mitochondrial oxidation. Stacking these two powerful lipolytic agents will flood the bloodstream with free fatty acids. If the subject is not engaging in high-volume, aerobic energy expenditure to burn these circulating lipids, the fatty acids will simply be redeposited, negating the biochemical synergy of the stack.
Sample Research Stacking Protocol
A theoretical clinical biohacking protocol designed for maximum lipid oxidation over an 8-week cycle often looks like this:
- AM (Fasted): 250 mcg AOD9604, followed immediately by 45 minutes of Zone 2 aerobic exercise to oxidize liberated lipids.
- Mid-Day (Fasted): 250 mcg AOD9604 to maintain localized lipolytic signaling.
- PM (Pre-Bed, Fasted): 1 mg to 2 mg Tesamorelin to induce nocturnal GH pulses for visceral fat targeting and systemic recovery.
10. Safety Profiles, Side Effects, and Contraindications
Common Side Effects of Tesamorelin
Because tesamorelin exerts a powerful, systemic neuroendocrine effect, its side effect profile is more pronounced.
- Injection Site Reactions: Erythema and pruritus (redness and itching) are common due to the lipophilic modification.
- Edema & Arthralgia: Water retention and joint pain are classic downstream effects of elevated growth hormone.
- Insulin Resistance: The most critical contraindication. Tesamorelin can elevate fasting blood glucose. It should be used with extreme caution in pre-diabetic or metabolically compromised subjects.
Common Side Effects of AOD9604
AOD9604 is globally recognized for its exceptional safety profile. Because it lacks somatogenic properties, it does not cause edema, joint pain, or insulin resistance. Side effects are typically confined to:
- Mild flushing or headache immediately post-injection.
- Minor injection site sensitivity.
Long-term Safety Data and Oncological Considerations
The starkest contrast between these peptides lies in oncological risk. Elevated IGF-1 (a byproduct of tesamorelin) is highly mitogenic; it promotes cellular division. Therefore, tesamorelin is strictly contraindicated in individuals with active malignancies or a history of cancer. AOD9604, possessing zero capacity to elevate systemic IGF-1, does not carry this proliferative risk, making it a vastly safer option for longevity-focused researchers analyzing long-term cellular health.
11. Legal Status and Sourcing: FDA Approval vs. Research Chemicals
Understanding Tesamorelin’s Prescription Status (Egrifta)
Tesamorelin holds the distinction of being an FDA-approved medication. Under the trade name Egrifta, it is legally prescribed by physicians specifically for HIV-infected patients suffering from lipodystrophy. Because it has official pharmaceutical status, clinical-grade tesamorelin is highly regulated. Outside of this specific prescription framework, it is sold strictly as a research chemical, not for human consumption.
AOD9604 as an Investigational Compound
AOD9604 does not currently hold FDA approval as a prescription medication. Interestingly, it previously obtained GRAS (Generally Recognized As Safe) status by the FDA for use as a dietary supplement or food additive. However, as an injectable peptide, it falls into the category of an investigational research compound or, in some specific clinical settings, an active pharmaceutical ingredient (API) utilized by compounding pharmacies under strict doctor-patient compliance.
How to Vet B2B Wholesale Suppliers for Research Quality
For laboratories acquiring these peptides, sourcing is everything. Validating a B2B supplier requires demanding specific documentation:
- Third-Party Certificates of Analysis (COA): Verifying >98% purity.
- Mass Spectrometry (MS) Reports: Ensuring correct molecular weight.
- Endotoxin Testing: Crucial for in vivo animal models to ensure the peptide is sterile and free from pyrogens.
12. Frequently Asked Questions (FAQs)
Q1: How long does it take to see weight loss results from AOD9604 vs Tesamorelin?
AOD9604 can initiate localized lipolysis almost immediately, with physical changes often measurable via skinfold calipers within 3-4 weeks. Tesamorelin requires systemic remodeling; noticeable reductions in deep visceral fat typically manifest around weeks 6-8, peaking at week 12.
Q2: Will AOD9604 build muscle like regular HGH?
No. AOD9604 lacks the specific amino acid sequence required to bind to the full growth hormone receptor. It does not stimulate the liver to produce IGF-1, meaning it has zero anabolic or muscle-building properties.
Q3: Does Tesamorelin cause insulin resistance?
It can. By elevating systemic growth hormone, tesamorelin increases circulating free fatty acids, which can competitively inhibit glucose uptake in muscles. Researchers must monitor fasting blood glucose during a cycle.
Q4: Which is better for belly fat specifically?
For subcutaneous belly fat (the soft fat you can pinch), AOD9604 is highly effective. For deep visceral belly fat (the hard fat beneath the muscle wall surrounding the organs), tesamorelin is clinically superior.
Q5: Do these peptides require PCT (Post Cycle Therapy)?
No. Unlike anabolic-androgenic steroids, neither AOD9604 nor tesamorelin suppresses the HPTA (Hypothalamic-Pituitary-Gonadal axis). Tesamorelin mimics natural GHRH, and once discontinued, the pituitary simply returns to its baseline secretory rhythm without the need for pharmacological recovery.
13. Key Takeaways
Summary of the Tesamorelin Profile
Tesamorelin is a powerhouse neuroendocrine signaling agent. By stimulating the pituitary to release robust, pulsatile waves of growth hormone, it is arguably the most effective peptide available for targeting dangerous visceral adipose tissue. However, its high efficacy is tied to a more complex side-effect profile, requiring diligent monitoring of systemic IGF-1 levels and glucose tolerance.
Summary of the AOD9604 Profile
AOD9604 is the ultimate precision tool for localized lipid oxidation. By extracting only the lipolytic fragment of the hGH molecule, it bypasses the pituitary entirely, acting directly on fat cells to liberate triglycerides while preventing new fat formation. Its lack of impact on IGF-1 and insulin makes it an exceptionally safe, highly tolerable compound for generalized fat loss.
Final Verdict for Researchers and Biohackers
When analyzing tesamorelin vs aod9604, the choice is dictated entirely by the biological target. B2B researchers studying metabolic syndrome, lipodystrophy, or deep visceral fat remodeling will prioritize the upstream, systemic power of tesamorelin. Conversely, advanced B2C biohackers seeking targeted subcutaneous fat reduction, longevity, and a pristine safety profile without anabolic risk will overwhelmingly favor the localized precision of AOD9604.