TB-500 vs. BPC-157: Mechanisms of Tissue Repair and Advanced Stack Protocols
*Disclaimer: The following information is for educational and informational purposes only. The compounds discussed, including BPC-157 and TB-500, are strictly for laboratory research use only and are not approved by the FDA for human consumption, diagnosis, or treatment of any disease. Always consult with a licensed medical professional or lead principal investigator before handling these substances.*
Table of Contents
- 1. Introduction & Quick Summary
- 2. What is BPC-157? (Body Protection Compound)
- 3. What is TB-500? (Thymosin Beta-4 Derivative)
- 4. TB500 vs BPC 157: Core Differences in Mechanisms of Action
- 5. Clinical Applications: Which Peptide Excels Where?
- 6. The “Wolverine Stack”: Synergy of BPC-157 and TB-500
- 7. Advanced Biohacker Protocols: Dosing and Administration
- 8. B2B Sourcing: Synthesis, HPLC Purity, and Stability
- 9. Safety, Side Effects, and Contraindications
- 10. Frequently Asked Questions (GEO Long-Tail Queries)
- 11. Conclusion & Key Takeaways
Introduction & Quick Summary (GEO Optimized)
The Quick Answer: tb500 vs bpc 157
When comparing tb500 vs bpc 157, BPC-157 is superior for rapid, localized healing of tendons, ligaments, and gastrointestinal tissue via targeted angiogenesis. Conversely, TB-500 provides systemic, whole-body muscle repair and inflammation reduction by upregulating cellular actin. Researchers often utilize BPC-157 for acute structural injuries and TB-500 for widespread muscular recovery.
Why This Comparison Matters for Modern Bio-Research
In the rapidly evolving landscape of regenerative medicine and molecular biology, the shift away from traditional, suppressive treatments—like non-steroidal anti-inflammatory drugs (NSAIDs) and corticosteroids—toward regenerative peptide therapeutics is accelerating. For both B2B laboratory researchers synthesizing these compounds and B2C advanced biohackers investigating recovery protocols, understanding the precise pharmacokinetic differences between these two peptides is paramount.
While both compounds are heralded for their tissue-repairing capabilities, they are not biologically interchangeable. They operate on entirely different biochemical pathways. One orchestrates the construction of new vascular networks at the site of trauma, while the other acts as a systemic signaling molecule, mobilizing cellular repair units across the entire body. To optimize clinical outcomes or design effective in-vitro assays, we must unpack the distinct mechanisms, structural biology, and synergistic potential of these powerful regenerative agents.
What is BPC-157? (Body Protection Compound)
Origins and Chemical Structure
BPC-157 (Body Protection Compound-157) is a synthetic pentadecapeptide, meaning it is comprised of a precise chain of 15 amino acids (sequence: Gly-Glu-Pro-Pro-Pro-Gly-Lys-Pro-Ala-Asp-Asp-Ala-Gly-Leu-Val). Fascinatingly, this sequence is a partial fragment of a much larger parent protein naturally found in human gastric juice.
Evolutionarily speaking, the stomach is an incredibly hostile environment, constantly subjected to highly acidic gastric acid (pH 1.5 to 3.5) and digestive enzymes. The parent protein of BPC-157 exists specifically to protect the mucosal lining of the stomach from digesting itself, rapidly repairing cellular damage and ulcerations. In a laboratory setting, synthesizing this specific 15-amino acid sequence isolates the purest regenerative properties of the gastric protein while maintaining remarkable chemical stability. It has a molecular weight of 1419.5 Daltons (Da) and, unlike many fragile peptides, exhibits extraordinary resilience to enzymatic degradation and heat stress.
Primary Mechanism: Angiogenesis and The NO System
The clinical efficacy of BPC-157 hinges on its profound ability to stimulate angiogenesis—the physiological process through which new blood vessels form from pre-existing vessels.
To achieve this, BPC-157 heavily upregulates Vascular Endothelial Growth Factor (VEGF), specifically enhancing the expression of VEGFR2 receptors. When tissue is damaged—particularly avascular tissue like tendons and ligaments, which notoriously lack blood flow—the healing process is strictly bottlenecked by the delivery of oxygen and nutrients. By aggressively stimulating the localized creation of capillary networks at the site of administration, BPC-157 bypasses this biological limitation.
Furthermore, BPC-157 acts as a potent modulator of the Nitric Oxide (NO) system. It influences Nitric Oxide Synthase (NOS) enzymes, ensuring endothelial cells (the cells lining the blood vessels) function optimally. This NO modulation not only aids in vasodilation (widening of the blood vessels for increased flow) but also mitigates localized oxidative stress and inflammation without suppressing the acute inflammatory response necessary for the initial stages of healing.
What is TB-500? (Thymosin Beta-4 Derivative)
Origins and Molecular Function
To understand TB-500, we must first look at its biological parent: Thymosin Beta-4 (Tβ4). Tβ4 is a naturally occurring, highly conserved 43-amino acid peptide produced by the thymus gland. It is found in high concentrations in blood platelets, wound fluid, and various tissues throughout the mammalian body, serving as one of the primary immune and tissue-repair signaling molecules triggered during acute trauma.
TB-500 is a synthetic version of this compound. In biochemical and pharmaceutical research, TB-500 traditionally refers to the active binding domain of Tβ4—specifically the peptide fragment containing amino acids 17-23 (LKKTETQ). This specific sub-sequence holds the active properties responsible for actin binding and cell migration. However, it is a crucial nuance for laboratory researchers sourcing wholesale peptides that many modern synthesis facilities produce the entire 43-amino acid Tβ4 sequence and label it commercially as TB-500. Regardless of whether a lab utilizes the fragment or the full chain, the physiological target remains the same: the cellular cytoskeleton.
Primary Mechanism: Actin Up-regulation and Cell Migration
The architectural foundation of every cell in the human body is the cytoskeleton, primarily composed of a protein called actin. Actin exists in two forms: G-actin (free-floating monomers) and F-actin (polymerized filaments). For a cell to move, divide, or repair tissue, it must constantly assemble and disassemble these actin filaments.
TB-500 functions as a highly potent actin-sequestering molecule. It binds to G-actin, preventing it from polymerizing into F-actin until it is precisely needed. By regulating this actin dynamic, TB-500 dramatically enhances cellular migration.
Think of it this way: if BPC-157 is building the roads (blood vessels) to the injury site, TB-500 is mobilizing the cellular construction workers (fibroblasts, myoblasts, and endothelial cells) and allowing them to travel vast distances through the body to reach the site of trauma. Because of its low molecular weight (approximately 4963 Da for the full sequence) and lack of binding to the extracellular matrix, TB-500 is entirely systemic. A subcutaneous injection in the abdomen will circulate and hunt down systemic inflammation and micro-tears in a strained shoulder, a torn hamstring, or an inflamed myocardium.
TB500 vs BPC 157: Core Differences in Mechanisms of Action
Localized Angiogenesis vs. Systemic Cellular Migration
The fundamental differentiator in the tb500 vs bpc 157 debate comes down to where and how they act. BPC-157 is highly localized. While it exerts some systemic effects (particularly concerning the gut and central nervous system), its primary regenerative mechanism—angiogenesis—is highly concentrated at the site of administration. If a researcher is modeling the repair of a specific, localized tear (e.g., a ruptured Achilles), BPC-157 introduced adjacent to the trauma yields targeted, hyper-accelerated vascularization.
TB-500, conversely, is a systemic patroller. Its mechanism of upregulating actin and reducing inflammatory cytokines (like TNF-alpha) occurs body-wide. It does not need to be administered near the site of injury. It excels at widespread tissue remodeling, muscle hypertrophy recovery, and modulating systemic immune responses.
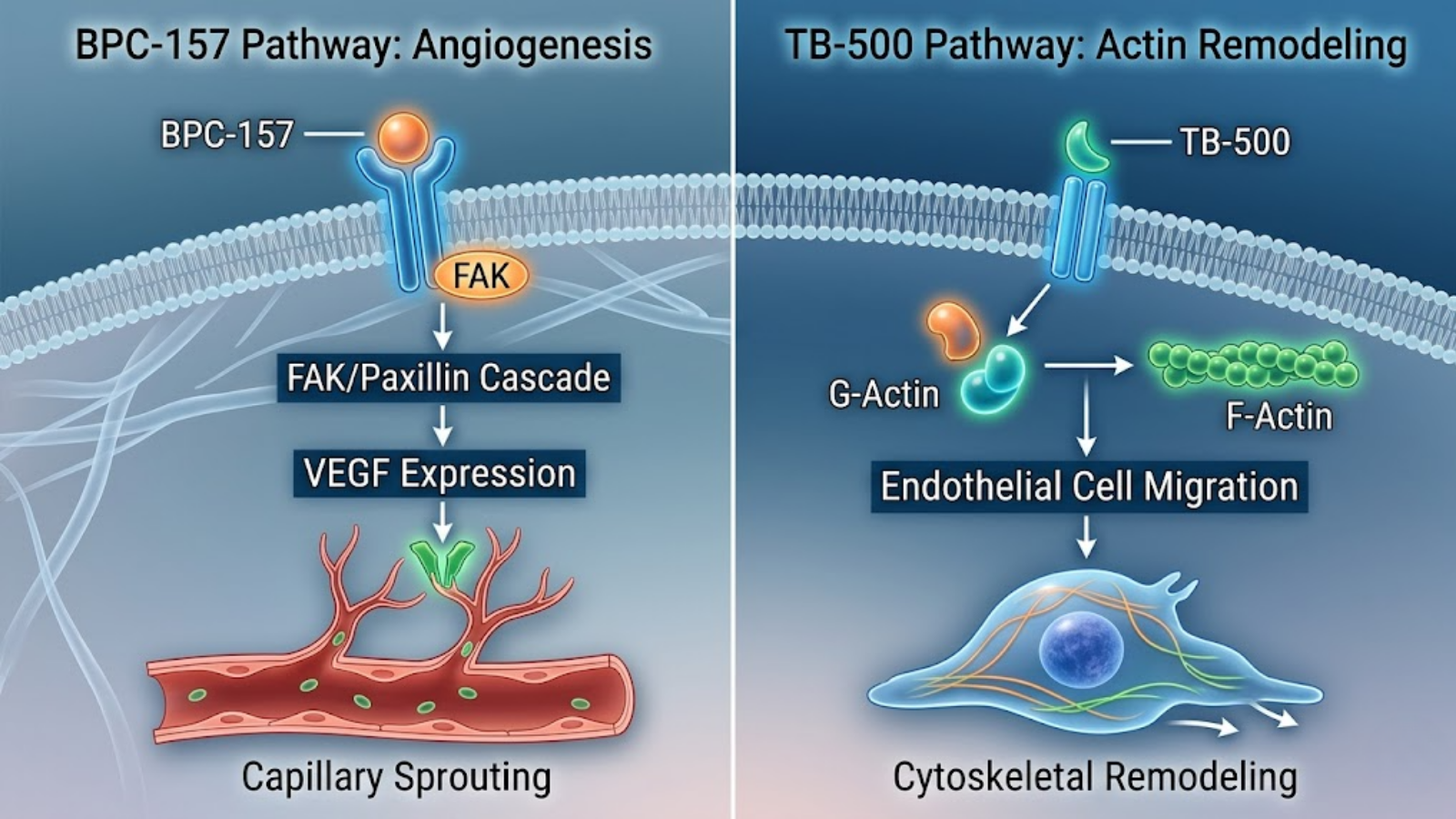
Fig 1. Conceptual visualization comparing TB-500’s systemic actin sequestering and BPC-157’s localized angiogenic stimulation.
Pharmacokinetics and Bioavailability
From a laboratory synthesis and administration standpoint, these peptides exhibit vastly different pharmacokinetic profiles. Because BPC-157 is derived from gastric juice, it is structurally designed to survive harsh environments. This gives it exceptional oral bioavailability. When synthesized as an arginate salt (BPC-157 Arginate), it can survive the GI tract and enter the bloodstream, making it highly effective for both systemic circulation and localized gut healing.
TB-500 is entirely degraded by gastric enzymes and possesses near-zero oral bioavailability. It must be administered parenterally (via subcutaneous or intramuscular injection) to enter systemic circulation. Furthermore, TB-500 has a much longer biological half-life, allowing for less frequent dosing protocols compared to the rapid metabolism of BPC-157.
Comparative Data: BPC-157 vs. TB-500
| Biochemical Property | BPC-157 (Body Protection Compound) | TB-500 (Thymosin Beta-4) |
|---|---|---|
| Amino Acid Length | 15 Amino Acids (Pentadecapeptide) | 43 Amino Acids (Full Tβ4) or 7 AA (Fragment) |
| Molecular Weight | 1419.5 Da | 4963 Da (Full sequence) |
| Primary Mechanism | VEGF Upregulation, Angiogenesis, NO Modulation | Actin Sequestration, Cellular Migration |
| Action Scope | Primarily Localized (with secondary systemic effects) | Entirely Systemic |
| Optimal Target Tissue | Tendons, Ligaments, Fascia, Gut Endothelium | Skeletal Muscle, Cardiac Tissue, Global Inflammation |
| Oral Bioavailability | High (especially in Arginate salt form) | Near Zero (Requires Injection) |
| Estimated Half-Life | Short (approx. 4 to 6 hours) | Long (approx. 24 to 72 hours) |
Clinical Applications: Which Peptide Excels Where?
Understanding the biomechanical and cellular pathways allows us to map these peptides to their highly specific clinical and practical applications.
Tendons, Ligaments, and Joint Repair
When analyzing connective tissue—tendons, ligaments, and cartilage—BPC-157 is the undisputed primary agent. Connective tissues are notoriously avascular; they have extremely poor blood supply. This is why a muscle tear heals in weeks, but a ligament tear (like an ACL or UCL) takes months or requires surgical intervention. BPC-157 induces the outgrowth of collateral blood vessels into these “dead zones,” heavily increasing the proliferation of tendon fibroblasts. In vitro studies consistently demonstrate that BPC-157 enhances the survival of fibroblasts under oxidative stress and accelerates the formation of Sharpey’s fibers—the structural matrix that anchors tendons to bone. For biohackers or clinical researchers dealing with chronic tendinopathy, tennis elbow, or rotator cuff tears, BPC-157 provides the localized vascular infrastructure required for regeneration.
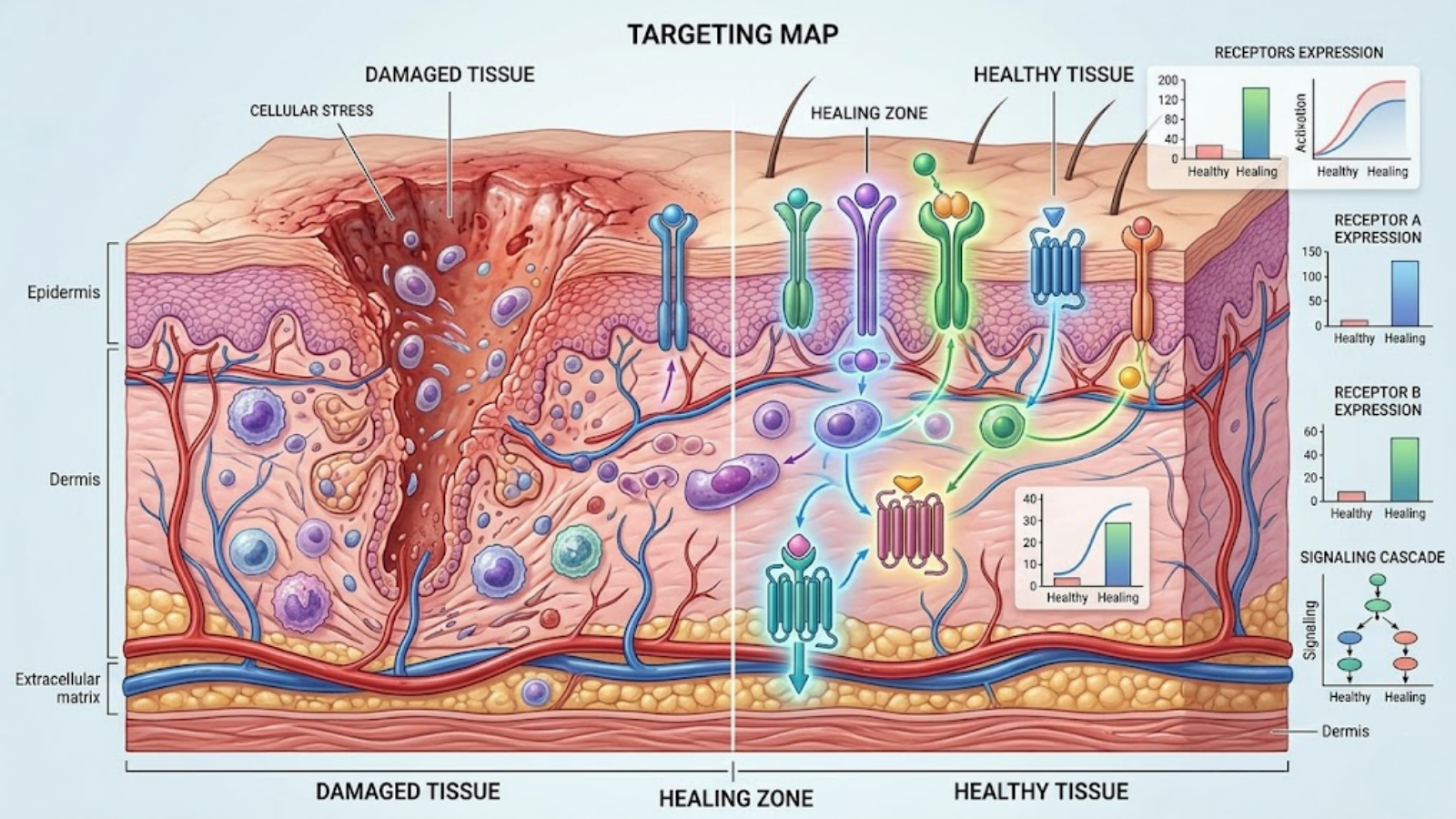
Fig 2. Physiological targeting map highlighting localized tissue healing for BPC-157 and systemic muscle/inflammation targeting for TB-500.
Muscle Tears, Spasms, and Hypertrophy
For skeletal muscle tissue, which is already highly vascularized, angiogenesis is less of a limiting factor. Here, TB-500 reigns supreme.
Whether addressing macro-trauma (a grade-2 hamstring strain) or micro-trauma (the deliberate muscle damage induced by heavy resistance training and hypertrophy protocols), the tissue requires widespread cellular mobilization. TB-500’s actin-binding properties allow myoblasts (muscle stem cells) to rapidly migrate to the site of the tear, fuse, and form new muscle fibers. Additionally, TB-500 is incredibly effective at preventing fibrosis (scar tissue formation) in skeletal muscle. By downregulating inflammatory cytokines and promoting healthy tissue regeneration rather than fibrotic patching, TB-500 ensures that the healed muscle retains its elasticity and contractile strength, preventing the tight, spasm-prone scar tissue often associated with severe muscular injuries.
Gastrointestinal and Neurological Healing
Beyond musculoskeletal applications, BPC-157 possesses profound and highly unique applications for the gastrointestinal tract and central nervous system. As a gastric peptide, it stabilizes the gut endothelium, maintaining tight junction integrity. It is heavily researched for its potential in reversing “leaky gut” (intestinal permeability), resolving gastric ulcers, and mitigating the symptoms of Inflammatory Bowel Disease (IBD).
Neurologically, BPC-157 interacts with both the dopaminergic and serotonergic systems. It exhibits neuroprotective properties, with animal models showing efficacy in protecting somatosensory neurons from neurotoxins and even aiding in the recovery of traumatic brain injuries (TBI) by modulating the inflammatory cascade within the brain. While TB-500 plays a role in neural repair—specifically in promoting the remyelination of damaged nerves—BPC-157 remains the superior compound for acute gastrointestinal and neuro-inflammatory interventions.
The “Wolverine Stack”: Synergy of BPC-157 and TB-500
Why Stack Them? The Compounding Effect
In the world of advanced tissue repair and performance longevity, it is rare to find two biological agents that complement each other with such precise physiological symmetry. This is why the combination of these two peptides—colloquially referred to in the biohacking community as the “Wolverine Stack”—has garnered immense traction.
To understand the compounding effect, we must look at the biological order of operations during wound healing. When a severe structural injury occurs (such as a torn rotator cuff or a ruptured patellar tendon), the localized tissue is starved of oxygen and vital nutrients due to compromised blood flow. BPC-157 acts as the master architect, upregulating VEGF and rapidly constructing a localized vascular network to bathe the injured tissue in blood.
However, blood flow alone is not enough if the body is not mobilizing enough cellular repair units to the site. This is where TB-500 enters the equation. By upregulating actin and enhancing cellular migration, TB-500 acts as a systemic dispatcher, flooding the newly built vascular “roads” with fibroblasts, myoblasts, and immune cells. Analyzing tb500 vs bpc 157 in isolation misses the broader clinical picture: BPC-157 creates the localized infrastructure, and TB-500 provides the systemic cellular labor. Together, they create a hyper-accelerated, synergistic healing environment that drastically outpaces the body’s baseline recovery capabilities.
Expected Timelines for Tissue Regeneration
While double-blind, placebo-controlled human trials remain scarce due to FDA classifications, in-vitro laboratory data, animal models, and extensive anecdotal clinical data from advanced biohackers paint a clear picture of expected regeneration timelines.
For grade 2 muscular strains or mild ligamentous sprains, baseline human recovery typically dictates a 4-to-6-week timeline before returning to load-bearing activities. When the synergistic stack is applied, structural stability and a massive reduction in localized pain are frequently reported within 10 to 14 days. It is a critical biomechanical caveat, however, that the suppression of pain and inflammation often outpaces the actual structural remodeling of the tendon. Therefore, researchers and athletes must exercise extreme caution to avoid re-injury by returning to peak physical loads before the new collagen matrix has fully cross-linked and solidified.
Advanced Biohacker Protocols: Dosing and Administration
*Disclaimer: The following dosing protocols are extrapolated from animal models and independent researcher data. They are presented for informational and educational purposes only. These compounds are not approved for human use.*
BPC-157 Dosing Strategies
Because of its short biological half-life (roughly 4 to 6 hours), BPC-157 requires frequent administration to maintain stable blood serum levels.
- Administration Route: For gastrointestinal or systemic neurological healing, oral administration (specifically the Arginate salt form) is highly effective at dosages of 250mcg to 500mcg daily. For structural trauma (tendons/ligaments), subcutaneous (SubQ) or intramuscular (IM) injection as close to the injury site as comfortably possible is the gold standard.
- Standard Dosage: The universally accepted research dosage is 250mcg to 500mcg, administered twice daily (e.g., once in the morning, once in the evening). This ensures continuous localized angiogenesis throughout the diurnal cycle.

Fig 3. Clinical flat lay demonstrating conceptual research-grade peptide vials, syringes, and clinical documentation for advanced protocols.
TB-500 Dosing Strategies
TB-500 has a significantly longer half-life, meaning it does not require daily administration. Its systemic nature also means that injection site proximity to the injury is largely irrelevant; a standard abdominal subcutaneous injection will circulate systemically.
- The Loading Phase: To reach therapeutic tissue saturation, researchers typically employ a “loading phase” for the first 4 to 6 weeks. The standard dosage here is 4mg to 6mg per week, usually split into two injections (e.g., 2mg on Monday, 2mg on Thursday).
- The Maintenance Phase: Once the acute injury has resolved, many biohackers transition to a maintenance protocol of 2mg once or twice a month to manage systemic inflammation and prevent re-injury.
Example Stack Protocol Ratios
A standard 6-week “Wolverine Stack” protocol for acute tendon or muscle rupture typically looks like this:
- Daily: 500mcg BPC-157 (injected SubQ near the injury site, split 250mcg AM / 250mcg PM).
- Bi-Weekly: 2.5mg TB-500 (injected SubQ in the abdomen, twice per week, for a total of 5mg weekly).
- Duration: 4 to 6 weeks, followed by a minimum 4-week washout (cessation) period to allow cellular receptor sensitivity to reset.
B2B Sourcing: Synthesis, HPLC Purity, and Stability
For laboratory procurement officers and principal investigators, the efficacy of the tb500 vs bpc 157 discussion is entirely moot if the raw materials are degraded or contaminated. Quality control is the bedrock of peptide research.
Understanding HPLC and Mass Spectrometry Testing
Synthesizing peptides is an incredibly complex biochemical process. During synthesis, amino acid sequences can truncate, misfold, or bind with chemical solvents like Trifluoroacetic acid (TFA), which is highly toxic to human and animal cells.
Legitimate wholesale suppliers must provide a Certificate of Analysis (COA) utilizing High-Performance Liquid Chromatography (HPLC) and Mass Spectrometry (MS).
- HPLC separates the components in a mixture to verify that the vial contains a minimum of 99% pure peptide, with less than 1% being synthesis byproducts.
- Mass Spectrometry verifies the exact molecular weight (e.g., confirming the BPC-157 sample weighs exactly 1419.5 Da). Anything less than 99% purity introduces severe experimental variables and safety risks.

Fig 4. A modern biotech laboratory verifying HPLC and Mass Spectrometry data for research-grade peptide purity.
Lyophilization and Reconstitution Protocols
Wholesale peptides are shipped as lyophilized (freeze-dried) powder. This process removes water under a vacuum, creating a stable chemical “puck” that prevents the amino acid bonds from degrading during transit.
To utilize the peptide, it must be reconstituted. For in-vivo models, the universal solvent is Bacteriostatic Water (BAC), which contains 0.9% benzyl alcohol. This prevents bacterial growth inside the vial once the vacuum seal is broken. The reconstitution process must be gentle; aggressively shooting water directly onto the lyophilized puck or shaking the vial can physically shear the delicate peptide bonds, rendering the compound inert.
Cold Chain Storage and Shelf Life
| Peptide State | Optimal Storage Temperature | Estimated Shelf Life |
|---|---|---|
| Lyophilized (Powder) | Freezer (-20°C / -4°F) | 24 to 36 months |
| Lyophilized (Powder) | Refrigerator (2°C to 8°C) | 12 to 18 months |
| Lyophilized (Powder) | Room Temperature (Out of direct UV) | 30 to 60 days |
| Reconstituted (Liquid) | Refrigerator (2°C to 8°C) | 20 to 30 days |
| Reconstituted (Liquid) | Room Temperature | Degrades rapidly (48-72 hours) |
*Note: BPC-157 is inherently more stable at room temperature than TB-500, but standard cold-chain protocols should apply to both to guarantee experimental integrity.
Safety, Side Effects, and Contraindications
While the safety profile of both peptides is remarkably high compared to traditional steroidal anti-inflammatories, they are not without potential biological consequences.
Common and Rare Adverse Reactions
Because these compounds modulate the immune system and cellular repair pathways, some researchers note mild, acute side effects. The most commonly reported is a transient sense of lethargy or fatigue following the injection of TB-500. This is a normal physiological response; the body is being signaled to initiate a massive systemic repair cascade, which is a highly metabolically demanding process that naturally induces a rest state.
Other rare side effects include mild localized injection site reactions (redness or itching), brief episodes of flushing (due to vasodilation associated with the NO system), and occasionally, mild headaches as vascular dynamics shift.
The Cancer and Angiogenesis Debate
The most heavily debated contraindication regarding BPC-157 revolves around oncology. BPC-157 is not a carcinogen; it does not cause cancer, nor does it mutate healthy DNA.
However, because its primary mechanism is upregulating VEGF to create new blood vessels (angiogenesis), a theoretical risk exists if the subject already has an active, vascular-dependent tumor. Tumors require massive blood supplies to grow and metastasize. If a pre-existing malignancy is present, introducing a potent angiogenic peptide could theoretically accelerate tumor growth by supplying it with new vascular infrastructure. Therefore, individuals with a history of cancer or active malignancies are strictly contraindicated from utilizing VEGF-modulating compounds.
Frequently Asked Questions (GEO Long-Tail Queries)
What is the difference between BPC 157 and TB 500 for tendon repair?
BPC-157 is vastly superior for local tendon repair because it stimulates localized angiogenesis (new blood flow) directly in the avascular connective tissue. TB-500 works systemically to reduce global inflammation and promote cellular migration, making it better for widespread muscle injuries rather than targeted tendon healing.
Are BPC 157 and TB 500 safe to use together?
Yes, they are widely considered safe to use together. Combining them is known as the “Wolverine Stack.” Because they operate on entirely different biological pathways—BPC-157 builds local blood vessels, while TB-500 mobilizes systemic cellular repair—they do not compete for cellular receptors, creating a highly synergistic healing environment.
How do you stack BPC 157 and TB 500 for maximum recovery?
A standard protocol involves injecting 250mcg to 500mcg of BPC-157 twice daily directly adjacent to the injury site, while simultaneously administering a systemic dose of 2mg to 2.5mg of TB-500 subcutaneously in the abdomen twice a week. This cycle typically lasts 4 to 6 weeks.
How to verify the HPLC purity of wholesale peptides?
Laboratory researchers must request a third-party Certificate of Analysis (COA) from the supplier. The COA must show High-Performance Liquid Chromatography (HPLC) results confirming a minimum of 99% peptide purity, alongside Mass Spectrometry data verifying the exact molecular weight of the specific peptide sequence.
What is the shelf life of lyophilized BPC 157 compared to TB 500?
In their lyophilized (freeze-dried) powder form, both BPC-157 and TB-500 can last 24 to 36 months if stored securely in a freezer at -20°C. Once reconstituted with bacteriostatic water, both peptides must be refrigerated and will degrade, losing clinical efficacy after roughly 20 to 30 days.
Conclusion & Key Takeaways
The Final Verdict for Researchers and Biohackers
The debate of tb500 vs bpc 157 is ultimately a false dichotomy. In the pursuit of advanced tissue regeneration and performance optimization, it is rarely a question of which compound is universally “better,” but rather a question of highly specific clinical application.
For the B2B laboratory researcher designing an in-vitro model for gastrointestinal repair or isolated ligamentous vascularization, BPC-157 is the precise biological tool required. For the researcher looking to modulate systemic inflammation, prevent muscular fibrosis, and study whole-body cellular migration, TB-500 is unmatched. And for the advanced B2C biohacker dealing with a devastating musculoskeletal injury, understanding that these peptides act as the localized “infrastructure” and the systemic “labor force,” respectively, unlocks the true potential of regenerative peptide therapeutics.
Summary of Key Takeaways
- BPC-157 acts locally, utilizing VEGF upregulation to create new blood vessels (angiogenesis) in tissue with poor blood flow, making it ideal for tendons, ligaments, and gut repair.
- TB-500 acts systemically, sequestering actin to promote the rapid migration of repair cells across the entire body, making it ideal for muscular trauma and global inflammation.
- Synergy is key: Stacking the two compounds yields compounding regenerative effects by simultaneously addressing localized blood flow bottlenecks and systemic cellular mobilization.
- Quality control is paramount: Laboratory synthesis requires rigorous HPLC and mass spectrometry testing to ensure 99%+ purity, as contaminants like TFA can ruin experimental data and cause cellular toxicity.
- Cold chain matters: Both compounds must be meticulously stored. Freeze lyophilized powders for long-term storage, and always refrigerate liquid vials immediately after reconstitution with bacteriostatic water.