Sermorelin vs. Tesamorelin vs. Ipamorelin: The Definitive Guide to Mechanisms, Purity, and Protocols
Sermorelin vs. Tesamorelin vs. Ipamorelin: The Definitive Guide to Mechanisms, Purity, and Protocols
Table of Contents
- Quick Answer: Sermorelin vs Tesamorelin vs Ipamorelin Summary
- Introduction: The Evolution of Growth Hormone Secretagogues
- Sermorelin: The Foundation of GHRH Therapy
- Tesamorelin: The Heavyweight for Visceral Fat and Lipodystrophy
- Ipamorelin: The Selective GHRP for Sleep and Recovery
- Head-to-Head: Sermorelin vs Tesamorelin vs Ipamorelin
- Purity, Synthesis, and Laboratory Analytics (B2B Focus)
- Clinical Protocols, Dosages, and Synergistic Stacking (B2C Focus)
- Safety Profiles, Side Effects, and Contraindications
- Frequently Asked Questions (GEO-Targeted Long-Tail Queries)
- Key Takeaways & Final Verdict
Quick Answer: Sermorelin vs Tesamorelin vs Ipamorelin Summary
When comparing sermorelin vs tesamorelin vs ipamorelin, the primary distinction lies in their receptor targets and physiological outcomes. Sermorelin acts as a baseline growth hormone-releasing hormone (GHRH) for generalized metabolic support. Tesamorelin is a structurally modified GHRH analog uniquely potent for aggressively targeting visceral fat. Conversely, ipamorelin is a growth hormone-releasing peptide (GHRP) that selectively enhances deep sleep and tissue recovery without elevating cortisol or prolactin levels.
The TL;DR Breakdown
- Sermorelin: The baseline anti-aging and vitality peptide; best for restoring natural, youthful growth hormone pulsatility without overstimulation.
- Tesamorelin: The heavyweight metabolic optimizer; highly specialized for aggressive visceral adipose tissue (VAT) reduction and improving lipid profiles.
- Ipamorelin: The selective recovery agent; ideal for sleep optimization, muscle repair, and athletic recovery, boasting the cleanest safety profile with zero cortisol spikes.
Introduction: The Evolution of Growth Hormone Secretagogues
To fundamentally understand the clinical applications of these compounds, we must first shift our perspective away from exogenous recombinant human growth hormone (rhGH) and look toward the endogenous somatotropic axis. Exogenous HGH administration, while highly anabolic, presents a significant biochemical flaw: it creates a negative feedback loop that effectively shuts down the pituitary gland’s natural production of GH, leading to somatotroph atrophy and tachyphylaxis (receptor downregulation).
This is where secretagogues represent a massive leap forward in both molecular biology and clinical biohacking. Instead of replacing growth hormone, secretagogues act upstream. They stimulate the anterior pituitary gland to secrete its own intrinsic stores of GH in a natural, pulsatile manner, thereby preserving the body’s homeostatic feedback mechanisms involving Insulin-like Growth Factor-1 (IGF-1) and somatostatin.
What Are Peptides and Secretagogues?
At the molecular level, a peptide is simply a short chain of amino acids linked by peptide bonds. When this chain exceeds 50 amino acids, it is generally classified as a protein. Secretagogues are highly specific classes of peptides engineered to trigger the secretion of another substance—in this case, growth hormone. The biological elegance of a secretagogue lies in its half-life and clearance rate; they enter the system, bind to highly specific transmembrane receptors, trigger an intracellular signaling cascade, and are subsequently degraded by proteolytic enzymes, leaving the body’s endocrine loop intact.
Conceptual microscopic visualization of GHRH vs. GHRP signaling pathways.
The Endogenous GH Axis: GHRH vs. GHRP
To grasp the nuances of sermorelin vs tesamorelin vs ipamorelin, one must understand that they operate on two completely distinct biological pathways.
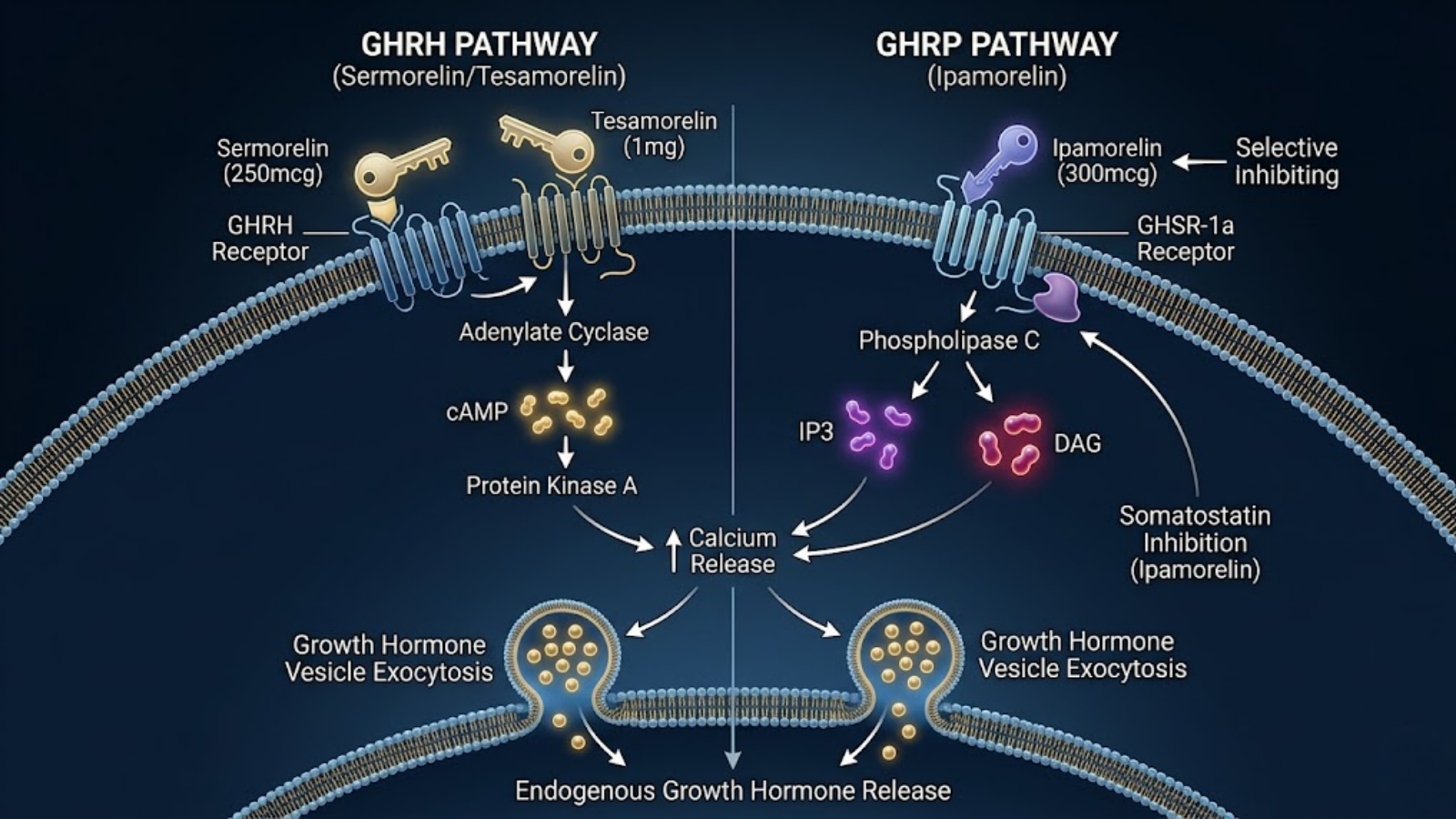
1. Growth Hormone-Releasing Hormones (GHRH): Both Sermorelin and Tesamorelin belong to this class. They bind directly to the GHRH receptor on the somatotroph cells in the pituitary. Mechanistically, this binding activates adenylate cyclase, leading to an accumulation of intracellular cyclic AMP (cAMP). This cAMP elevation opens calcium channels, triggering the exocytosis (release) of pre-synthesized growth hormone vesicles.
2. Growth Hormone-Releasing Peptides (GHRP): Ipamorelin belongs to this class. GHRPs are ghrelin mimetics. They do not bind to the GHRH receptor; instead, they bind to the Growth Hormone Secretagogue Receptor (GHSR-1a). This binding triggers a completely different secondary messenger system involving phospholipase C, which increases intracellular inositol triphosphate (IP3) and diacylglycerol (DAG), ultimately leading to a massive synergistic release of GH while simultaneously inhibiting somatostatin (the hormone responsible for halting GH release).
| Feature | GHRH (Sermorelin, Tesamorelin) | GHRP (Ipamorelin) |
|---|---|---|
| Primary Receptor | GHRH-R (Pituitary Somatotrophs) | GHSR-1a (Ghrelin Receptor) |
| Intracellular Messenger | cAMP / Protein Kinase A | IP3 / DAG / Calcium release |
| Somatostatin Effect | Susceptible to somatostatin block | Inhibits somatostatin activity |
| Synergistic Potential | High (when paired with a GHRP) | High (when paired with a GHRH) |
Sermorelin: The Foundation of GHRH Therapy
Sermorelin (historically marketed under the brand name Geref) is the undisputed grandfather of modern peptide therapy. It is the bio-identical, truncated version of naturally occurring human Growth Hormone-Releasing Hormone. Researchers and optimized-aging clinics often rely on clinical-grade sermorelin as a fundamental building block for foundational metabolic support.
Mechanism of Action (The 29-Amino Acid Chain)
Endogenous, naturally occurring GHRH is a 44-amino acid polypeptide. However, decades of biochemical assaying revealed that the entire 44-chain is not necessary for receptor activation. The biological activity—the actual “key” that unlocks the GHRH receptor on the pituitary gland—resides entirely within the first 29 amino acids at the N-terminus.
Therefore, Sermorelin was synthesized as GRF 1-29 (Growth Hormone-Releasing Factor 1-29). Because it is an exact structural match to the bioactive portion of natural GHRH, it binds with perfect affinity to the GHRH receptor. It operates exclusively by elevating intracellular cAMP, inducing a natural, physiologic pulse of growth hormone that mimics the exact amplitude and frequency seen in healthy young adults.
Primary Clinical Outcomes
In both clinical practice and B2C biohacking protocols, Sermorelin is utilized for foundational metabolic support. It is rarely the choice for rapid, aggressive body recomposition. Instead, its clinical outcomes are marked by subtle, long-term systemic improvements.
Researchers consistently observe a gradual enhancement in skin elasticity and collagen density (due to downstream IGF-1 upregulation), improved deep-wave sleep parameters, a mild reduction in general adiposity, and an overall restoration of vitality. It is the ultimate baseline peptide—often prescribed in optimized-aging clinics to bring a 50-year-old’s GH pulsatility back to the physiological levels of a 30-year-old.
Pharmacokinetics and Half-Life
From a laboratory and B2B synthesis perspective, sermorelin‘s defining characteristic is its incredibly short biological half-life. Once injected subcutaneously, Sermorelin is rapidly cleaved by dipeptidyl peptidase-IV (DPP-IV) and other plasma proteases. Its half-life in the human body is roughly 11 to 12 minutes.
This rapid clearance means timing is absolutely critical. It must be administered on a strictly empty stomach (as insulin completely blunts natural GH release) and is typically dosed immediately prior to sleep to align with and amplify the body’s largest natural nocturnal growth hormone pulse.
Tesamorelin: The Heavyweight for Visceral Fat and Lipodystrophy
If Sermorelin is a general practitioner, Tesamorelin is a highly specialized surgeon. Tesamorelin is a synthetic analogue of GHRH, but it has been structurally modified to bypass the exact pharmacokinetic limitations that hold Sermorelin back. It is widely recognized in the advanced biohacking community as a potent metabolic intervener, specifically for visceral fat accumulation.
Mechanism of Action and FDA Heritage
Structurally, Tesamorelin is identical to the 44-amino acid sequence of human GHRH, but with a critical, proprietary modification at the N-terminus: the addition of a trans-3-hexenoic acid group.
This seemingly minor biochemical tweak radically alters the molecule’s behavior. The trans-3-hexenoic acid acts as a shield, making the peptide highly resistant to enzymatic degradation by DPP-IV. As a result, Tesamorelin has a significantly extended half-life and binding affinity compared to Sermorelin. This stability allows it to exert a much stronger, more sustained agonistic effect on the pituitary somatotrophs. Its potency is so well-documented that under the brand name Egrifta, Tesamorelin earned FDA approval for the treatment of HIV-associated lipodystrophy (a condition characterized by severe, dangerous accumulation of visceral fat around the organs).
Lipogenesis Inhibition vs. Targeted Lipolysis
Tesamorelin is widely regarded in the advanced biohacking community as the most potent peptide available for body recomposition, specifically targeting Visceral Adipose Tissue (VAT).
Unlike subcutaneous fat (the soft fat just beneath the skin), visceral fat wraps around the internal organs and is highly metabolically active, driving systemic inflammation and insulin resistance. Tesamorelin attacks VAT through two distinct mechanisms: 1. Targeted Lipolysis: The massive pulses of GH triggered by Tesamorelin directly bind to adipocyte (fat cell) receptors, upregulating hormone-sensitive lipase (HSL) and breaking down stored triglycerides into free fatty acids to be oxidized for energy. 2. Lipogenesis Inhibition: It actively blunts the formation of new fat cells in the visceral cavity.
Clinical data repeatedly demonstrates that tesamorelin can reduce visceral adipose tissue by upwards of 15-20% over a 12 to 26-week protocol, an outcome unmatched by almost any other compound short of extreme caloric restriction or GLP-1 agonists. Furthermore, it reliably improves lipid profiles, lowering circulating triglycerides.
The Ideal Candidate Profile
In both clinical environments and the B2C sector, Tesamorelin is not utilized for basic anti-aging. It is deployed for targeted metabolic intervention. The ideal candidate is an individual struggling with stubborn trunk adiposity, visceral fat accumulation, or a researcher aiming to observe rapid shifts in lipid metabolism and body composition parameters.
Ipamorelin: The Selective GHRP for Sleep and Recovery
Transitioning away from the GHRH class, we arrive at Ipamorelin, widely considered the crown jewel of the Growth Hormone-Releasing Peptide (GHRP) category. When exploring sermorelin vs tesamorelin vs ipamorelin, it is vital to understand that Ipamorelin acts on an entirely different receptor system, making its safety profile and effects highly unique. Advanced biohackers frequently prioritize Ipamorelin protocols specifically for neurological recovery and sleep optimization.
Mechanism of Action (The Clean Ghrelin Agonist)
Ipamorelin is a synthetic pentapeptide (composed of five amino acids: Aib-His-D-2-Nal-D-Phe-Lys-NH2). As a GHRP, it is a ghrelin mimetics. Ghrelin, known colloquially as the “hunger hormone,” binds to the GHSR-1a receptor in the brain, triggering profound growth hormone release while simultaneously shutting down somatostatin.
However, earlier generations of GHRPs (like GHRP-6 and GHRP-2) came with severe side effects: ravenous, uncontrollable hunger (gastric emptying) and unintended stimulation of the adrenal and thyroid axes. Ipamorelin was meticulously engineered to strip away these side effects. It is highly selective, binding to the ghrelin receptor to trigger a slow, sustained pulse of GH without activating the extreme hunger pathways associated with its predecessors.
Zero Cortisol and Prolactin Impact
What makes ipamorelin the darling of both laboratory researchers and biohackers is its remarkable selectivity. In clinical pharmacology, a “dirty” drug binds to multiple unintended receptors. Ipamorelin is the “cleanest” GHRP in existence.
Even at saturation doses, Ipamorelin does not stimulate the release of ACTH (Adrenocorticotropic hormone), cortisol (the primary stress hormone), or prolactin. Elevated cortisol drives muscle breakdown and fat storage, while elevated prolactin can cause gynecomastia and suppressed testosterone. By leaving these hormones completely untouched, Ipamorelin allows for pure growth hormone elevation without the endocrine collateral damage seen with other peptides.
Deep Sleep Architecture and Tissue Repair
Because of its clean profile and sustained half-life (~2 hours), Ipamorelin is heavily utilized for central nervous system recovery and sleep optimization.
When administered subcutaneously before bed, Ipamorelin profoundly alters sleep architecture. EEG data on GHRPs show a distinct prolongation of Slow-Wave Sleep (SWS)—the deepest, most restorative stage of sleep where the brain clears neurotoxic waste and the body initiates cellular repair. For athletes, bodybuilders, and executives, Ipamorelin serves as the ultimate recovery protocol. It accelerates the healing of micro-tears in muscle fascia, improves ligament integrity, and ensures that the central nervous system recovers fully overnight, all without the visceral fat-melting aggression of Tesamorelin or the rapid clearance limitations of Sermorelin.
Head-to-Head: Sermorelin vs Tesamorelin vs Ipamorelin
To construct an optimal clinical or research protocol, one must analyze the comparative pharmacodynamics of these secretagogues. When evaluating **sermorelin vs tesamorelin vs ipamorelin**, researchers must weigh the intended outcome—whether it be generalized endocrine support, aggressive lipid oxidation, or selective neurological recovery—against the molecular half-life and receptor affinity of each peptide.
The following matrix delineates the core clinical and molecular differentiators:
| Clinical Metric / Biomarker | Sermorelin (GHRH 1-29) | Tesamorelin (Modified GHRH) | Ipamorelin (GHRP) |
|---|---|---|---|
| Primary Receptor Target | Pituitary GHRH Receptor | Pituitary GHRH Receptor | GHSR-1a (Ghrelin Receptor) |
| Biological Half-Life | Extremely short (~11-12 mins) | Extended (~30-45 mins) | Extended (~120 mins) |
| Visceral Fat Loss Potency | Low to Moderate | Exceptionally High | Moderate |
| Impact on Deep Sleep (SWS) | Moderate | Low to Moderate | Exceptionally High |
| Cortisol/Prolactin Elevation | None | None | None (Highly Selective) |
| Somatostatin Inhibition | No | No | Yes |
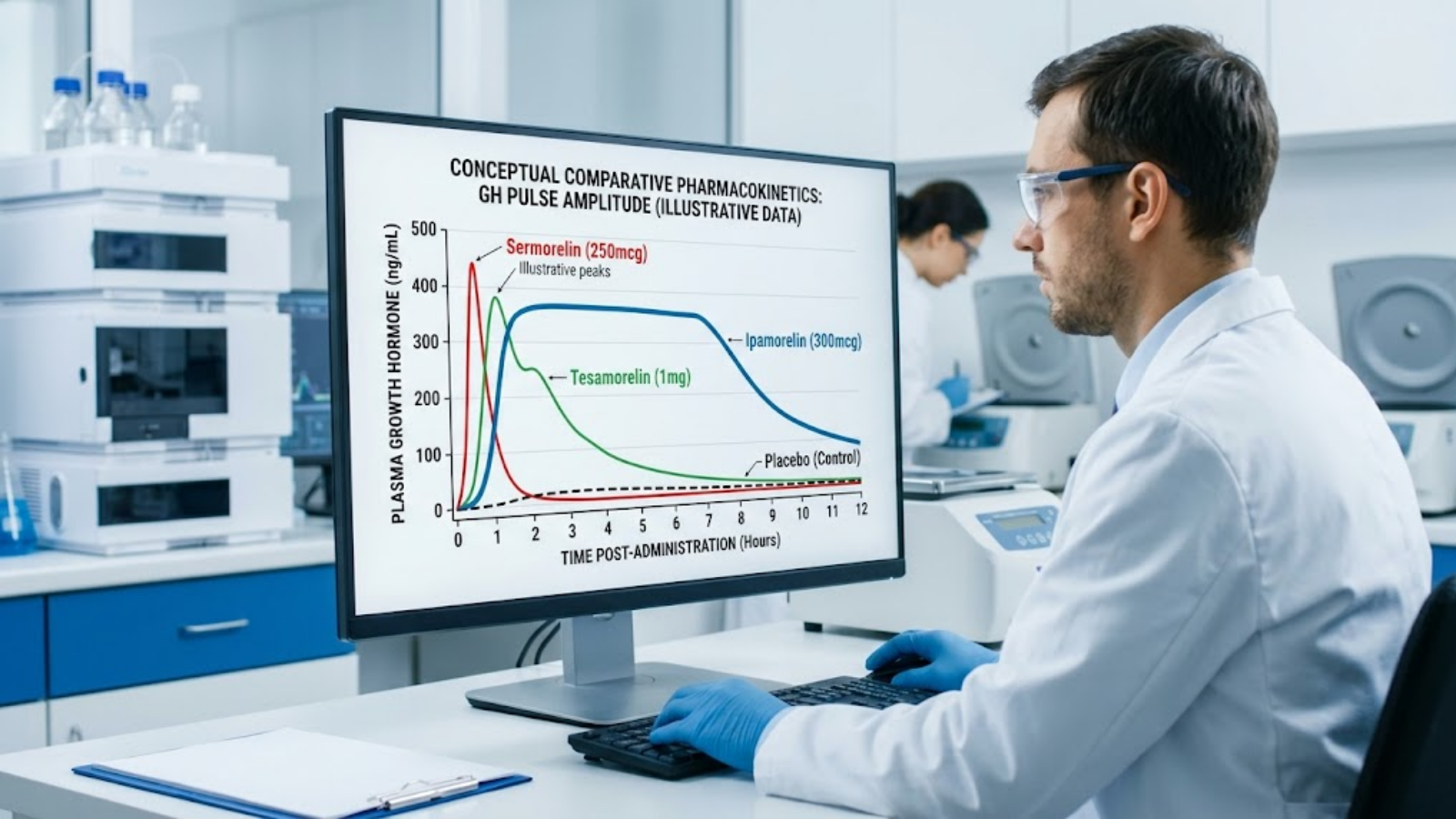
Conceptual comparative pharmacokinetic data illustrating pulse amplitude and half-life.
Efficacy in Body Composition and Fat Loss
If the primary endpoint is the reduction of Visceral Adipose Tissue (VAT), Tesamorelin is unequivocally the superior compound. Its extended half-life and resistance to enzymatic cleavage allow for a sustained pulse of growth hormone that violently upregulates hormone-sensitive lipase (HSL) within adipocytes. Sermorelin will assist in general body composition over a 6-to-12-month horizon by slowly elevating baseline IGF-1, but it lacks the lipolytic aggression of Tesamorelin. Ipamorelin falls in the middle; while it does not target visceral fat as aggressively as Tesamorelin, it preserves lean muscle mass effectively and facilitates a favorable metabolic environment for fat loss without stimulating the hunger pathways that derail dietary compliance.
Impact on Sleep Architecture and Recovery Metrics
For central nervous system (CNS) repair and athletic recovery, Ipamorelin is the gold standard. By agonizing the ghrelin receptor, it profoundly extends the duration of slow-wave sleep (SWS). Researchers tracking biometric data (such as HRV and deep sleep duration via wearables) consistently note immediate, measurable improvements with Ipamorelin. Sermorelin provides a mild sleep benefit due to its restoration of nocturnal GH pulsatility, while Tesamorelin is rarely utilized specifically for sleep enhancement.
Cost-to-Benefit Ratio in Clinical Settings
Sermorelin remains the most cost-effective option for long-term, low-dose anti-aging protocols. Because Tesamorelin requires complex synthesis (adding the trans-3-hexenoic acid group) and holds an FDA-approved heritage, it is significantly more expensive to procure for research or clinical use. Ipamorelin sits at a highly favorable cost-to-benefit intersection, offering profound physiological benefits with an impeccable safety profile at a moderate price point.
Purity, Synthesis, and Laboratory Analytics (B2B Focus)
For compounding pharmacies, procurement officers, and lead researchers, the efficacy of a peptide is entirely dependent on molecular integrity. The synthetic production of amino acid chains is fraught with potential for truncation, oxidation, and deamidation. Laboratory synthesis protocols must prioritize rigorous analytical verification to ensure compound stability and clinical potency.
The Importance of HPLC Purity and Mass Spectrometry
When sourcing research chemicals, verifying High-Performance Liquid Chromatography (HPLC) and Mass Spectrometry (MS) data is non-negotiable. HPLC separates the components of a synthesized batch to quantify the exact purity of the target peptide, while Mass Spectrometry verifies the molecular weight to ensure the sequence is flawless. A clinical-grade secretagogue should reflect a minimum HPLC purity of 99.0%. Impurities often consist of truncated peptide sequences (missing amino acids) which can cause unpredictable immune responses or simply render the compound biologically inert.
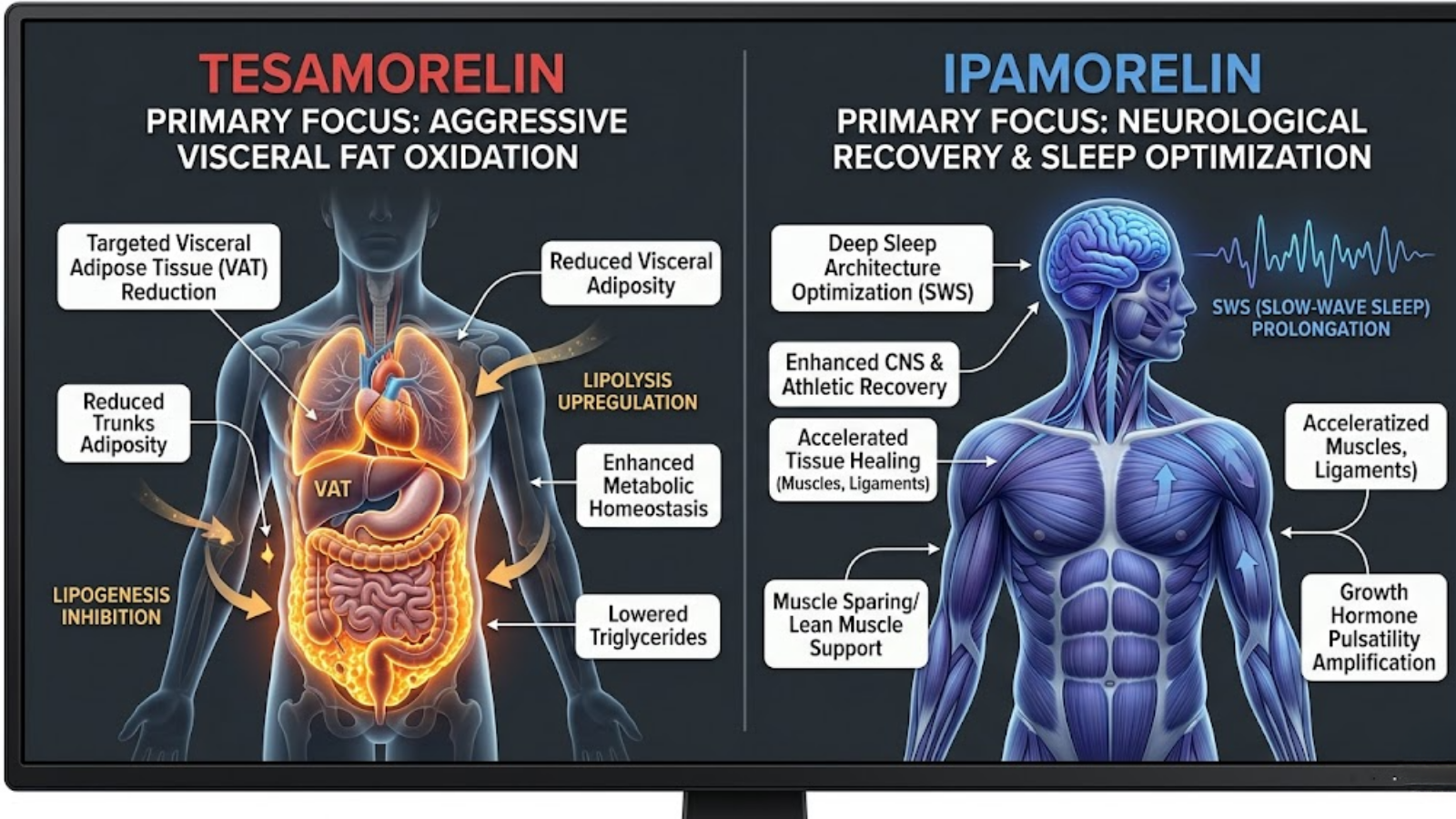
Comparative map of visceral fat reduction vs. deep sleep optimization.
Lyophilization and Molecular Stability
Peptides are incredibly fragile in an aqueous state. Therefore, they are subjected to lyophilization—a highly controlled freeze-drying process that sublimates water out of the vial under a vacuum, leaving behind a stable, solid “puck” of peptide salts (often bound to acetate or trifluoroacetate). The molecular weight of the peptide dictates its stability; Tesamorelin, being a larger 44-amino acid structure with a lipid-like attachment, requires strict temperature controls during lyophilization to prevent steric hindrance and degradation.
Reconstitution and Cold Chain Storage Protocols
Once lyophilized peptides are reconstituted using bacteriostatic water (water containing 0.9% benzyl alcohol to inhibit bacterial growth), the clock starts ticking on molecular degradation.
Agitation: Peptides must never be shaken. Violent agitation causes peptide bond cleavage and shearing. The bacteriostatic water should be dripped gently down the side of the vial.
Cold Chain: Post-reconstitution, all three peptides must be kept refrigerated between 2°C and 8°C (36°F – 46°F). Sermorelin and Ipamorelin generally remain stable for up to 30 days in solution, whereas Tesamorelin may begin to degrade in efficacy closer to the 14-to-21-day mark due to its structural complexity.
Clinical Protocols, Dosages, and Synergistic Stacking (B2C Focus)
In advanced biohacking and clinical optimization, secretagogues are rarely utilized haphazardly. Dosing is highly calculated, and compounds are frequently stacked to exploit biological synergy. Advanced metabolic clinicians often design protocols that alternate these secretagogues or incorporate potent tissue-specific recovery agents, such as IGF-DES, to optimize mitochondrial function and athletic performance outcomes.
General Monotherapy Dosing Guidelines
*Clinical note: Dosages in research literature vary widely based on the subject’s baseline endocrine function. The following represents standard observed ranges in clinical trials.*
- Sermorelin: Typically researched in ranges of 200mcg to 300mcg administered subcutaneously once daily, usually 30-60 minutes before bed.
- Tesamorelin: Because of its large molecular weight, clinical doses (such as those used in Egrifta trials) are significantly higher, often ranging from 1mg to 2mg daily, usually administered in the morning or split into two daily doses for maximum lipolytic action.
- Ipamorelin: Generally administered at 100mcg to 300mcg per dose. For sleep architecture optimization, a single pre-bedtime dose is standard. For athletic tissue repair, researchers often split the dose (morning, post-workout, and pre-bedtime).
The Synergy of Stacking: Blending GHRH and GHRP
The most advanced application of these peptides involves stacking a GHRH (Sermorelin or Tesamorelin) with a GHRP (Ipamorelin). Biologically, these two classes of drugs operate synergistically, not additively.
If a GHRH causes a growth hormone pulse of magnitude “2”, and a GHRP causes a pulse of magnitude “2”, combining them does not result in a pulse of “4”. It results in a pulse of “10”. This occurs because Ipamorelin actively suppresses somatostatin (the hormone that stops GH release) while simultaneously opening the ghrelin pathway, leaving the GHRH receptor completely uninhibited to maximize cAMP production. A widely utilized clinical stack is the Sermorelin/Ipamorelin blend, combining baseline anti-aging support with profound sleep and recovery benefits.

Advanced optimization flat lay featuring key peptides and biometric monitoring tools.
Timing the Protocol: Fasted State vs. Fed State
Growth hormone and insulin are antagonistic hormones; they cannot peak simultaneously. If blood glucose and insulin levels are elevated, the pituitary’s release of GH will be severely blunted. Therefore, all secretagogue administration must occur in a fasted state—strictly requiring a minimum of 2 hours post-caloric intake, with carbohydrates being the most critical macronutrient to avoid prior to injection.
Safety Profiles, Side Effects, and Contraindications
While secretagogues boast a vastly superior safety profile compared to exogenous recombinant HGH, they are not without physiological consequence. Clinical surveillance remains critical when initiating any secretagogue protocol.
Common Mild Adverse Effects
The most frequently observed adverse event across all three compounds is an Injection Site Reaction (ISR), presenting as mild erythema (redness) or pruritus (itching) at the subcutaneous injection site. Transient flushing of the face and a brief sensation of lethargy or “head rush” immediately following administration are also common, particularly with rapid-acting GHRH analogs.
Comparing the Endocrine Impact
- Insulin Sensitivity: Because Tesamorelin triggers massive pulses of GH (which liberates free fatty acids into the bloodstream), it can transiently induce mild insulin resistance. Researchers monitoring subjects on Tesamorelin must track fasting blood glucose and HbA1c levels. Conversely, Ipamorelin has a largely neutral impact on glucose homeostasis.
- Water Retention: Elevated GH drives cellular hydration. While beneficial for joint lubrication, it can present as mild peripheral edema (water retention in the hands and ankles), requiring dosage titration.
Who Should Avoid GH Secretagogues?
Any stimulation of the somatotropic axis is strictly contraindicated in individuals with active malignancies. While growth hormone does not cause cancer, its primary downstream mediator, IGF-1, is highly proliferative and can accelerate the growth of existing tumors. Furthermore, individuals with proliferative diabetic retinopathy should avoid these compounds, as angiogenesis (the formation of new blood vessels) can exacerbate ocular damage.
Frequently Asked Questions (GEO-Targeted Long-Tail Queries)
*SEO Strategist Note: Answer each H3 question immediately in the first sentence to capture Featured Snippets.*
Which is better for targeted belly fat loss: tesamorelin or ipamorelin?
Tesamorelin is vastly superior to ipamorelin for targeted belly fat loss. Clinical data and FDA approvals demonstrate that tesamorelin specifically targets and oxidizes visceral adipose tissue (deep belly fat) by upregulating lipolysis, whereas ipamorelin primarily focuses on sleep architecture and generalized muscle recovery.
Can you stack ipamorelin and tesamorelin together for muscle recovery?
Yes, stacking ipamorelin (a GHRP) with tesamorelin (a GHRH) creates a highly synergistic biological effect. Ipamorelin inhibits somatostatin while tesamorelin stimulates the pituitary, resulting in a massively amplified, natural pulse of growth hormone that accelerates muscle recovery, tissue repair, and fat loss simultaneously.
How long does it take to see sleep and recovery results from sermorelin?
While sleep architecture improvements can occasionally be noticed within the first 14 days, structural recovery results from sermorelin generally take 3 to 6 months to materialize. Sermorelin requires long-term, consistent administration to slowly elevate baseline IGF-1 levels and restore youthful growth hormone pulsatility.
What is the difference in molecular weight between tesamorelin and sermorelin?
The difference in molecular weight is substantial: tesamorelin is a larger, 44-amino acid sequence with an added trans-3-hexenoic acid group, while sermorelin is a much smaller, truncated 29-amino acid sequence. This structural difference gives tesamorelin a significantly longer biological half-life and greater stability.
How to verify the HPLC purity of synthesized GHRH peptides?
To verify the HPLC purity of synthesized GHRH peptides, you must request a third-party Certificate of Analysis (COA) from the synthesis laboratory. The COA will display a chromatogram; researchers should ensure the primary peak indicates a minimum of 99.0% purity, devoid of truncated or degraded peptide fragments.
Key Takeaways & Final Verdict
Navigating the biochemical nuances of growth hormone secretagogues requires precision, clear objectives, and an understanding of pharmacodynamics. The choice between these compounds relies entirely on aligning the molecular mechanism with the desired clinical outcome.
Summary of the Core Decision Matrix
- Choose Sermorelin if: Your objective is baseline, long-term anti-aging support. It is the ideal, cost-effective entry point for restoring youthful endocrine function, improving skin elasticity, and subtly enhancing vitality over a 6-to-12-month timeline.
- Choose Tesamorelin if: You are executing an aggressive metabolic intervention. If the primary goal is the rapid reduction of stubborn visceral adipose tissue, lowering triglycerides, and dramatic body recomposition, Tesamorelin’s extended half-life and lipolytic potency make it the undisputed choice.
- Choose Ipamorelin if: Your focus is on elite recovery, central nervous system repair, and sleep optimization. Because it acts selectively on the ghrelin receptor without spiking cortisol or hunger, it is the safest, cleanest peptide for athletes and executives looking to maximize deep slow-wave sleep and protect lean muscle mass.