Sermorelin vs. NAD+: Which Protocol Drives Better Cellular Regeneration and Longevity Outcomes?
Disclaimer: The information provided in this article is for educational, clinical, and informational purposes only. Certain compounds discussed, including specific peptides, may be designated for Laboratory Research Use Only and are not approved by the FDA for human consumption or dietary supplement use. Always consult a licensed, board-certified healthcare provider before undertaking any new therapeutic, clinical, or advanced biohacking protocol.
Sermorelin vs. NAD+: Which Protocol Drives Better Cellular Regeneration and Longevity Outcomes?
Table of Contents
- 1. Quick Answer: Sermorelin vs. NAD+
- 2. Introduction: The Intersection of Peptides and Coenzymes
- 3. Understanding NAD+: The Mitochondrial Engine of Cellular Repair
- 4. Understanding Sermorelin: The Endocrine Modulator for Recovery
- 5. Clinical Data: Which Drives Better Longevity Outcomes?
- 6. Delivery Methods and Bioavailability
- 7. Advanced Biohacking: Stacking Protocols
- 8. B2B Considerations: Wholesale Acquisition
- 9. Safety, Side Effects, and Contraindications
- 10. Frequently Asked Questions
- 11. Key Takeaways
1. Quick Answer: Sermorelin vs. NAD+
When evaluating sermorelin vs nad+, the core distinction lies in their biological targets. NAD+ is a critical coenzyme that fuels mitochondrial ATP production and activates DNA-repairing sirtuins. Conversely, sermorelin is a GHRH peptide that stimulates endogenous growth hormone release for systemic tissue repair and muscle preservation. For immediate cellular energy, NAD+ excels; for holistic structural recovery, sermorelin leads.
2. Introduction: The Intersection of Peptides and Coenzymes in Longevity
The landscape of advanced clinical therapeutics and longevity science has fundamentally shifted over the last decade. We are no longer merely managing the downstream symptoms of metabolic decline; instead, clinical researchers and advanced biohackers are targeting the upstream molecular drivers of the aging process itself. When we examine the recognized “Hallmarks of Aging”—specifically mitochondrial dysfunction, genomic instability, and altered intercellular communication—two specific compounds consistently emerge at the forefront of regenerative medicine: Nicotinamide Adenine Dinucleotide (NAD+) and Sermorelin.
Shifting the Paradigm of Anti-Aging
Historically, the anti-aging paradigm relied on exogenous hormone replacement, which often triggered severe negative feedback loops, shutting down the body’s endogenous production. Today, the focus is on restoration and precursor optimization. The goal is to provide the raw cellular machinery and the precise neuroendocrine signaling required for the body to repair itself. This is where the intersection of vital coenzymes (which govern intracellular energy) and secretagogue peptides (which govern systemic endocrine signaling) becomes paramount.
Defining the Scope: From Laboratory Bench to Clinical Protocol
To truly understand these compounds, we must bridge the gap between B2B biochemical synthesis and B2C clinical application. For laboratory researchers, wholesale compounders, and synthesis labs, the conversation revolves around molecular stability, high-performance liquid chromatography (HPLC) purity, and lyophilization techniques. For the advanced biohacker and the longevity clinician, the focus shifts to pharmacokinetics, bioavailability, receptor affinity, and synergistic stacking protocols. This comprehensive analysis will dissect both the structural chemistry and the clinical efficacy of these highly sought-after molecules.
3. Understanding NAD+: The Mitochondrial Engine of Cellular Repair
Nicotinamide Adenine Dinucleotide (NAD+) is not a hormone; it is a ubiquitous pyridine nucleotide coenzyme found in every living cell. It is arguably the most critical molecule in the human body aside from water, serving as the fulcrum for cellular metabolism and genomic maintenance.
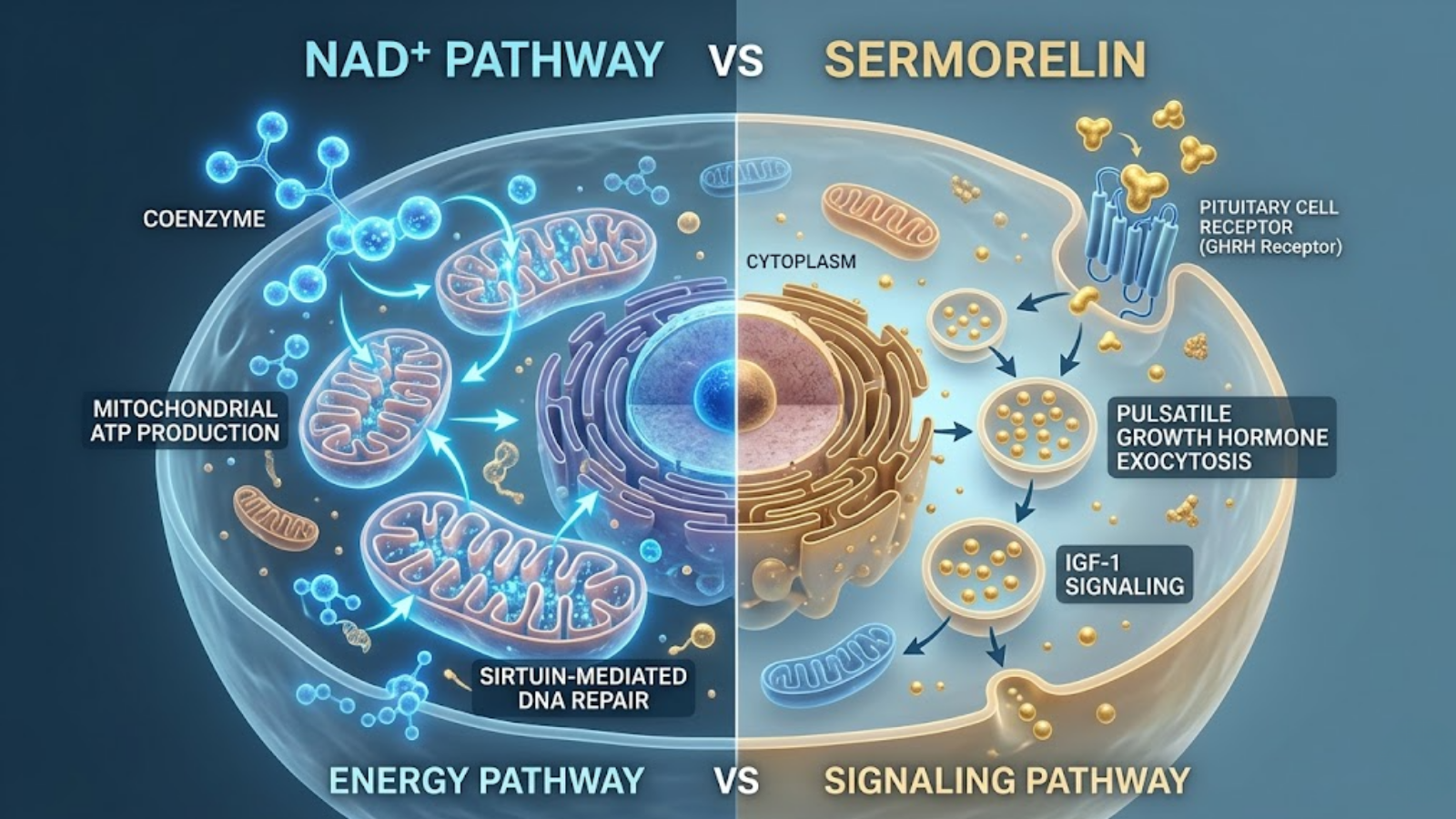
Fig 1: The Duality of Action – Energy production via the NAD+ mitochondrial pathway vs. Endocrine signaling via the Sermorelin/Pituitary pathway.
Mechanism of Action: The Redox Shift and Sirtuin Activation
At its core, NAD+ exists in two forms: an oxidized state (NAD+) and a reduced state (NADH). It functions primarily as a hydride acceptor and donor in redox reactions. Within the mitochondria, NAD+ is essential for the function of Complex I in the electron transport chain (ETC), directly driving the oxidative phosphorylation required to generate Adenosine Triphosphate (ATP)—the energy currency of the cell.
However, its role extends far beyond simple energy metabolism. NAD+ acts as a critical, consumable substrate for three primary classes of longevity-associated enzymes:
- Sirtuins (SIRT1-7): Often referred to as “longevity genes,” these NAD+-dependent deacetylases regulate cellular health, mitigate oxidative stress, and manage apoptosis. Sirtuins cannot function without an adequate pool of NAD+.
- Poly (ADP-ribose) polymerases (PARPs): These enzymes detect and initiate repair of single-strand DNA breaks. Overactive PARPs, often triggered by excessive UV exposure or environmental toxins, rapidly deplete cellular NAD+ stores.
- CD38 (Cyclic ADP-ribose hydrolases): Immune cells, particularly macrophages, express high levels of CD38 as we age. CD38 is a voracious consumer of NAD+, driving chronic low-grade inflammation (often termed “inflammaging”).
The Decline with Age: The NAD+ Deficit
The most pressing clinical issue regarding NAD+ is its severe age-related depletion. By the time a human reaches the age of 50, their systemic NAD+ levels have typically fallen by 50% compared to their baseline at age 20. This decline is a dual-edged sword: the body produces less NAD+ through the salvage pathway (mediated by the rate-limiting enzyme NAMPT), while simultaneously consuming more NAD+ due to the age-related upregulation of PARPs (repairing accumulated DNA damage) and CD38 (driving systemic inflammation). This deficit results in mitochondrial uncoupling, cellular senescence, and the physical manifestations of aging.
B2B Sourcing & Chemistry: The Laboratory Perspective
For researchers and wholesale pharmaceutical buyers, synthesizing and maintaining raw NAD+ presents unique chemical challenges. Pure NAD+ powder is highly hygroscopic, meaning it rapidly absorbs moisture from the air, which can lead to rapid degradation of the molecular structure.
| Biochemical Parameter | Laboratory Specification | Clinical Implication |
|---|---|---|
| Molecular Weight | 663.43 g/mol | Requires specific delivery vectors (IV, liposomal) due to size. |
| Solubility | Highly soluble in aqueous solutions. | Ideal for liquid IV compounding but risks rapid hydrolysis if not cold-chained. |
| Stability | Highly susceptible to heat, light, and moisture. | Mandates strict cold-chain shipping (-20°C) and amber vial storage. |
| Purity Standard | >98% via HPLC (High-Performance Liquid Chromatography). | Ensures absence of residual heavy metals and unreacted solvents from synthesis. |
Laboratories sourcing bulk, lyophilized NAD+ must demand rigorous third-party Certificates of Analysis (COAs). If the cold chain is broken during transit, the NAD+ can degrade into nicotinamide (NAM) and ADP-ribose, rendering the compound therapeutically inert and potentially inhibitory to sirtuin function.
4. Understanding Sermorelin: The Endocrine Modulator for Recovery
While NAD+ dictates intracellular energy, sermorelin operates on a macro, systemic level. Sermorelin (specifically Sermorelin Acetate) is a synthetic analog of naturally occurring Growth Hormone-Releasing Hormone (GHRH). It is a highly truncated peptide consisting of the first 29 amino acids of the endogenous 44-amino acid GHRH molecule, retaining full biological activity.
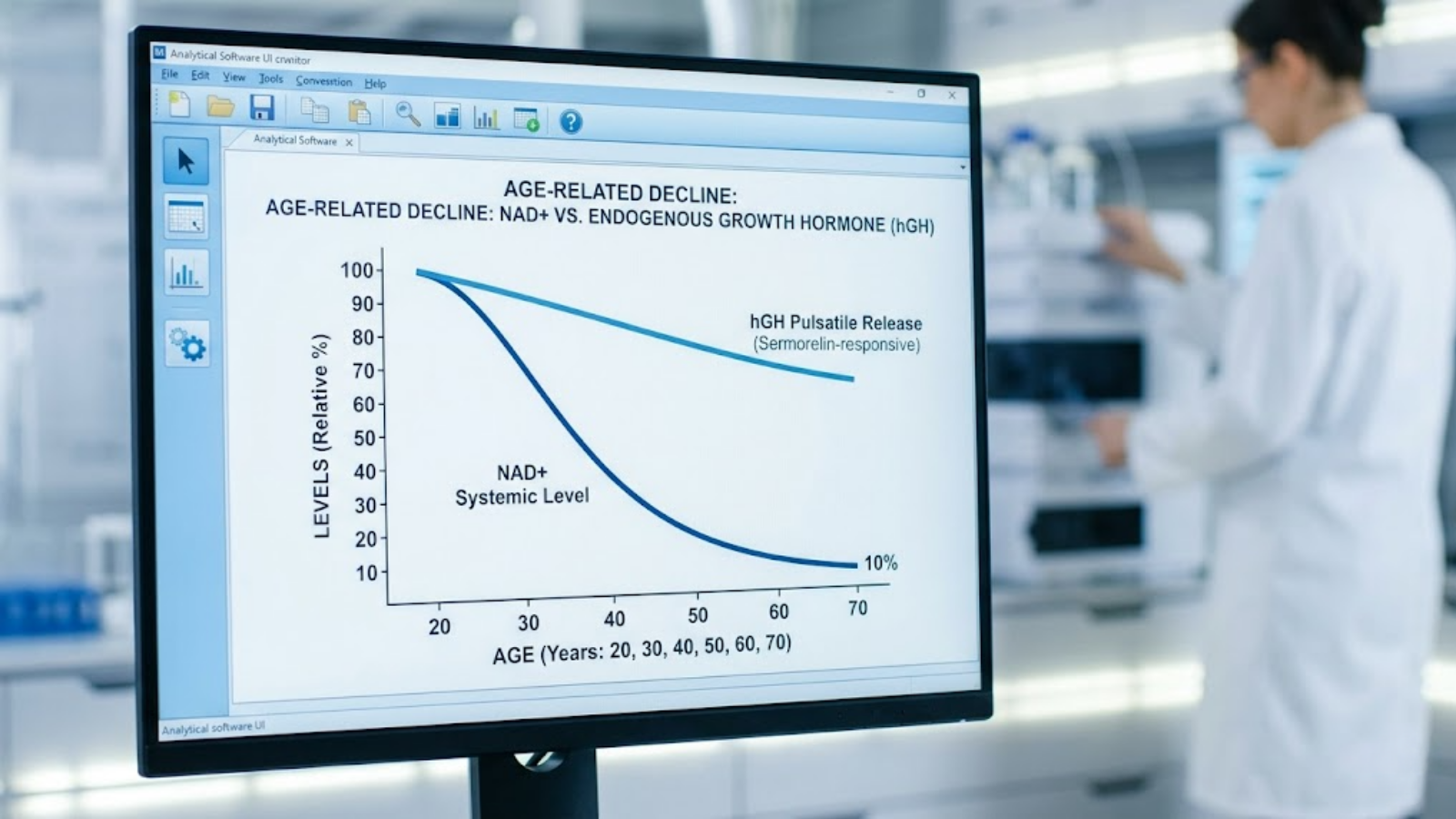
Fig 2: The Aging Decline – Clinical tracking mapping the systemic collapse of NAD+ alongside the progressive reduction in endogenous hGH pulses.
Mechanism of Action: The Somatotrope Stimulator
Unlike synthetic human growth hormone (rhGH), which floods the system and suppresses the body’s natural production, sermorelin acts strictly as a secretagogue. It binds specifically to the GHRH receptors located on the somatotrope cells in the anterior pituitary gland.
Upon binding, sermorelin triggers a highly regulated intracellular cascade: it activates adenylyl cyclase, which increases intracellular cyclic AMP (cAMP). This upregulates Protein Kinase A (PKA), leading to an influx of calcium ions (Ca2+). This calcium spike triggers the exocytosis of pre-packaged secretory vesicles containing endogenous human growth hormone (hGH) into the bloodstream. Because sermorelin relies on the body’s natural machinery, it preserves the critical pulsatile release of hGH and respects the negative feedback loop mediated by somatostatin, severely reducing the risk of tachyphylaxis (receptor downregulation) and acromegaly associated with exogenous hGH abuse.
The Role of IGF-1: The Anabolic Engine
The hGH released via sermorelin stimulation travels directly to the liver, where it acts as the primary catalyst for the production of Insulin-like Growth Factor 1 (IGF-1). IGF-1 is the primary mediator of growth hormone’s anabolic effects. It is responsible for stimulating chondrocyte (cartilage) proliferation, increasing osteoblast activity (bone density), promoting myoblast differentiation (muscle growth), and accelerating the lipolysis of visceral adipose tissue.
| Physiological Metric | Synthetic hGH Administration | Sermorelin Protocol |
|---|---|---|
| Mechanism | Direct receptor agonism | Stimulates endogenous pituitary production |
| Release Pattern | Non-pulsatile (“square wave” flood) | Natural, pulsatile physiological spikes |
| Negative Feedback | Suppresses pituitary function | Intact (regulated by somatostatin) |
| Tachyphylaxis Risk | High (receptor downregulation) | Extremely Low |
| Primary Clinical Use | Severe deficiency, muscle wasting | Anti-aging, optimized sleep, injury recovery |
Laboratory Insights: Peptide Synthesis and Purity
For the B2B laboratory sector, the synthesis of a 29-amino acid chain requires highly sophisticated Solid-Phase Peptide Synthesis (SPPS). Sermorelin is incredibly fragile. The peptide bonds are highly susceptible to enzymatic cleavage, deamidation, and oxidation—particularly at the methionine residue located at position 27.
When researchers procure lyophilized sermorelin acetate in bulk, it appears as a sterile white puck within a glass vial. To ensure stability, it must be reconstituted utilizing bacteriostatic water (water containing 0.9% benzyl alcohol) to prevent microbial growth. Even when reconstituted, the aqueous solution must be refrigerated between 2°C and 8°C and utilized within 30 days, as the peptide structure will actively degrade at room temperature, losing its binding affinity for the pituitary receptors.
5. Clinical Data: Which Drives Better Longevity Outcomes?
When evaluating the clinical data, advanced biohackers often ask: “Which is better for longevity?” The answer requires a nuanced understanding of what you are trying to heal. NAD+ and sermorelin do not compete; they govern entirely distinct biological jurisdictions.
NAD+ for Telomere Health, DNA Repair, and Neuroprotection
The clinical literature overwhelmingly supports NAD+ as the superior molecule for addressing the genomic hallmarks of aging. Intracellular NAD+ restoration has been shown to heavily influence the activity of SIRT6, a specific sirtuin critical for maintaining telomere length and stabilizing the genome.
Furthermore, robust clinical trials in neurodegenerative models demonstrate that maintaining high NAD+ pools prevents the energetic collapse of neurons. By keeping the mitochondrial electron transport chain highly efficient, NAD+ drastically reduces the leakage of Reactive Oxygen Species (ROS)—the free radicals that cause oxidative stress and lipid peroxidation. For a patient or biohacker suffering from “brain fog,” chronic fatigue syndrome, or post-viral mitochondrial dysfunction, clinical data indicates that NAD+ therapies yield a significantly faster and more direct restorative outcome than any secretagogue.
Sermorelin for Body Composition, Sleep Architecture, and Systemic Healing
Conversely, sermorelin dominates the clinical data regarding structural recovery. Aging is accompanied by a severe decline in slow-wave sleep (Delta sleep), the specific sleep phase where the majority of nocturnal hGH is secreted.
Clinical applications of sermorelin, administered subcutaneously prior to bedtime, demonstrate a profound ability to restore youthful hGH pulses. This leads to measurable improvements in body composition. Data tracking IGF-1 biomarkers over a 6-to-12-month sermorelin protocol consistently shows significant decreases in visceral adipose tissue (body fat) alongside simultaneous increases in lean muscle mass. Furthermore, the localized repair of musculoskeletal injuries—such as tendinopathies, ligament tears, and post-surgical recovery—is heavily reliant on the collagen synthesis pathways activated by sermorelin-induced IGF-1 release.
The Verdict on Cellular Regeneration Outcomes
| Target Outcome | Superior Protocol | Physiological Rationale |
|---|---|---|
| Genomic Stability / DNA Repair | NAD+ | Direct substrate required for PARP activation. |
| Lean Muscle Accretion | Sermorelin | Upregulates hepatic IGF-1 synthesis. |
| Mitochondrial ATP Production | NAD+ | Essential hydride transporter in Complex I of ETC. |
| Deep Sleep Restoration | Sermorelin | Enhances slow-wave (Delta) sleep architecture. |
| Neuroinflammation Reduction | NAD+ | Downregulates CD38 and activates SIRT1 pathways. |
Ultimately, if the goal is to correct cellular exhaustion at the molecular level, NAD+ is the scientifically backed intervention. If the goal is to reverse the physical, structural, and metabolic decay associated with somatopause (the age-related decline in growth hormone), sermorelin provides a safer, more sustainable mechanism than traditional hormone replacement.
6. The Great Debate: Delivery Methods and Bioavailability
Understanding the physiological mechanisms of these compounds is only half the battle. For both B2B laboratory compounders and B2C clinicians, the most critical variable in determining therapeutic efficacy is bioavailability—the proportion of the administered substance that successfully enters systemic circulation and reaches the target receptor sites. When comparing the pharmacokinetics of sermorelin vs nad+, the delivery protocols diverge significantly due to their distinct molecular weights and metabolic pathways.

Fig 3: Physiological Targeting Map – Showcasing systemic distribution, indicating how NAD+ heavily targets neuroprotection and liver function, while Sermorelin targets musculoskeletal anabolism.
NAD+ Delivery: Bypassing First-Pass Metabolism
The intact NAD+ molecule is a relatively large, highly charged dinucleotide. Because of its size and polarity, it cannot easily cross the cellular membrane of enterocytes (intestinal cells) without being cleaved into its precursor components, such as Nicotinamide Riboside (NR) or Nicotinamide Mononucleotide (NMN). Consequently, oral administration of pure NAD+ yields negligible systemic bioavailability due to aggressive enzymatic breakdown in the gastrointestinal tract and subsequent first-pass metabolism in the liver.
To achieve therapeutic intracellular concentrations, longevity clinics employ alternative vectors:
- Intravenous (IV) Infusion: This is the gold standard for immediate, high-dose systemic saturation. IV protocols typically range from 250mg to 1000mg infused over 2 to 4 hours. This bypasses the digestive tract entirely, forcing the coenzyme into the bloodstream to rapidly replenish depleted cellular reservoirs.
- Subcutaneous (SubQ) / Intramuscular (IM) Injections: For advanced biohackers seeking at-home protocols, SubQ injections offer a highly bioavailable, though lower-dose, alternative to IV drips. It provides a steady, controlled release into the capillaries.
- Oral Precursors (NMN/NR): While not intact NAD+, taking liposomal precursors allows the body to utilize the salvage pathway to synthesize NAD+ intracellularly. This is generally used for baseline maintenance rather than acute clinical intervention.
Sermorelin Pharmacokinetics: The Subcutaneous Imperative
Sermorelin acetate, like nearly all peptide therapeutics, is notoriously fragile. If ingested orally, the highly acidic environment of the stomach, combined with proteolytic enzymes like pepsin and trypsin, will completely cleave the 29-amino acid chain into biologically useless fragments within minutes.
Therefore, sermorelin must be administered via subcutaneous injection, typically into the adipose tissue of the abdomen. This allows the peptide to be slowly absorbed into the microvasculature.
- Circadian Timing: The most critical aspect of sermorelin delivery is timing. Endogenous hGH is not secreted in a steady stream; it is released in massive, pulsatile spikes, primarily during the first few hours of slow-wave (Delta) sleep. To respect and enhance this physiological rhythm, sermorelin protocols rigorously mandate nighttime injections, usually 30 to 60 minutes before bed. This administration effectively “primes” the pituitary somatotropes, resulting in a robust, naturally synchronized release of growth hormone that aligns with the body’s deeply ingrained circadian biology.
| Compound | Optimal Delivery Vector | Bioavailability | Circadian Timing | Primary Limitation |
|---|---|---|---|---|
| NAD+ | Intravenous (IV) Infusion | 100% (Systemic) | Morning/Mid-day | Time-consuming, clinical setting required. |
| Sermorelin | Subcutaneous (SubQ) Injection | High (90%+) | Nighttime (pre-sleep) | Requires strict cold-chain storage and reconstitution. |
7. Advanced Biohacking: Stacking Sermorelin and NAD+
In the elite tiers of longevity medicine and biohacking, clinicians rarely rely on a single monotherapy. The current frontier involves multi-pathway intervention. When analyzing sermorelin vs nad+, the most advanced clinical perspective is to recognize that they are not mutually exclusive. In fact, they are highly synergistic.

Fig 4: The Optimized Longevity Protocol – A clinical flat lay demonstrating the synergy of injectable sermorelin acetate paired with oral NAD+ precursors and sleep cycle tracking.
The Synergistic Approach: Energy and Signal
To understand the synergy, one must look at the body as a complex machine requiring both an operational signal and the energy to execute that signal. Sermorelin provides the powerful endocrine signal (via hGH and IGF-1) instructing the body to synthesize new tissue, repair collagen, and burn visceral fat. However, these anabolic processes are incredibly energy-intensive; they require vast amounts of ATP to drive cellular division and protein synthesis.
If a patient possesses the endocrine signal (via sermorelin) but suffers from age-related mitochondrial dysfunction and ATP depletion, the physical healing response will be blunted. By stacking NAD+ with sermorelin, the biohacker simultaneously upgrades the mitochondrial engine (NAD+) while turning the ignition key for tissue repair (sermorelin).
Sample Protocols for Optimization Clinics
A typical advanced stacking protocol respects the circadian rhythm of both compounds:
- AM Protocol (The Energy Phase): NAD+ administration (either via a low-dose SubQ injection or high-dose liposomal precursor) immediately upon waking. This floods the mitochondria with the necessary redox substrates to drive daytime ATP production, clear brain fog, and activate sirtuins for DNA repair.
- PM Protocol (The Recovery Phase): Sermorelin acetate (typically 200mcg to 300mcg) injected subcutaneously 30 minutes before sleep, ideally on an empty stomach to prevent insulin spikes from blunting the hGH release. This drives the nocturnal anabolic repair processes using the energy stores optimized by the morning NAD+.
8. B2B Considerations: Wholesale Acquisition and Laboratory Testing
For commercial laboratories, wholesale peptide suppliers, and compounding pharmacies, the acquisition and synthesis of these molecules represent rigorous biochemical challenges. Purity, stability, and exact molecular sequencing are non-negotiable parameters.
HPLC Purity Testing and Mass Spectrometry
Whether synthesizing a dinucleotide like NAD+ or a 29-amino acid chain like sermorelin, the manufacturing process yields impurities. In peptide synthesis (SPPS), truncated sequences (where an amino acid fails to attach) or deletion sequences frequently occur.
Laboratories must utilize High-Performance Liquid Chromatography (HPLC) coupled with Mass Spectrometry (MS) to verify the final product. A standard B2B Certificate of Analysis (COA) must demonstrate a purity of ≥98%. In the context of sermorelin vs nad+, impurities in sermorelin can trigger rapid immune responses (antibody formation against the peptide), while impurities in bulk NAD+ powders usually indicate the presence of residual organic solvents or heavy metal catalysts used during biosynthesis.
Storage and Thermal Stability Logistics
Cold-chain logistics strictly dictate the wholesale acquisition of these compounds:
- Lyophilized Sermorelin: Shipped as a freeze-dried powder, it is stable at room temperature for brief transit periods but should be stored at -20°C for long-term B2B storage. Once reconstituted with bacteriostatic water, it must be kept at 2°C to 8°C (refrigerated) to prevent rapid degradation of the methionine residue.
- Liquid NAD+ Formulations: Clinical-grade IV NAD+ solutions are highly unstable when exposed to heat and UV light. B2B shippers utilize insulated thermal packaging with calibrated cold packs to ensure the temperature never exceeds 8°C during transit, preventing the compound from aggressively hydrolyzing back into base nicotinamide.
9. Safety, Side Effects, and Contraindications
While both interventions boast exceptional safety profiles compared to synthetic hormones or heavy pharmaceuticals, they exert profound physiological effects and carry distinct, recognizable side effect profiles that clinicians must actively manage.
Managing the “NAD+ Flush”
The most prominent side effect associated with NAD+ is the infamous “NAD+ flush.” When NAD+ is infused intravenously too rapidly, the sudden surge of ATP production and the rapid shift in cellular redox states can trigger a systemic physiological response. Patients frequently report intense pressure or tightness in the chest, a sensation of breathlessness, cramping in the gastrointestinal tract, and intense flushing of the skin.
- Clinical Mitigation: This is not an allergic reaction; it is a rapid physiological metabolic shift. It is immediately mitigated by slowing the IV drip rate. Advanced biohackers utilizing SubQ NAD+ may experience a mild, localized version of this flush, which subsides within 10 to 15 minutes.
Sermorelin Injection Site Reactions and Sensitivities
Because sermorelin requires daily subcutaneous administration, the most common adverse events are Injection Site Reactions (ISRs). These present as localized erythema (redness), pruritus (itching), or mild induration (hardening) at the injection site. Furthermore, because sermorelin acts on the pituitary to stimulate hGH, some patients experience temporary lethargy, mild water retention, or flushed skin post-injection as the neuroendocrine axis adjusts to the secretagogue.
Oncological Considerations: The Growth Pathway Warning
The most critical contraindication for sermorelin therapy revolves around oncology. By definition, sermorelin upregulates hGH and, subsequently, IGF-1. IGF-1 is a potent mitogen—it stimulates cellular division and growth. Therefore, sermorelin is strictly contraindicated in patients with active malignancies or a high genetic predisposition to certain cancers, as the systemic elevation of IGF-1 could theoretically accelerate tumor proliferation. Conversely, NAD+ (via its role in DNA repair and PARP activation) is heavily researched for its potential genomic stabilization effects, though oncology patients should never initiate NAD+ protocols without direct oncological oversight.
10. Frequently Asked Questions (GEO Targeted)
Should I take sermorelin or NAD+ for mitochondrial repair and longevity?
For direct mitochondrial repair, NAD+ is scientifically superior. NAD+ acts as the essential coenzyme for the electron transport chain, directly fueling cellular ATP production and activating sirtuins for DNA repair. Sermorelin is better suited for structural, muscular, and hormonal longevity rather than intracellular mitochondrial optimization.
Can you safely stack subcutaneous NAD+ injections with sermorelin?
Yes, you can safely stack them, and it is a preferred protocol in advanced biohacking. Because they target entirely different pathways—NAD+ restoring intracellular energy and sermorelin stimulating systemic endocrine repair—they work synergistically. Typically, NAD+ is administered in the morning for energy, while sermorelin is injected at night.
What is the difference in degradation rates between lyophilized sermorelin and NAD+?
Lyophilized sermorelin is highly fragile and degrades rapidly upon reconstitution; it must be kept refrigerated and used within 30 days. Lyophilized bulk NAD+ is extremely hygroscopic and will aggressively degrade into nicotinamide if exposed to moisture or heat, mandating strict cold-chain logistics for B2B shipping.
How long does it take to feel cellular energy improvements from NAD+ versus sermorelin?
NAD+ provides highly immediate effects; IV infusions or SubQ injections can yield noticeable improvements in mental clarity and cellular energy within hours to days. Sermorelin requires a cumulative endocrine shift, meaning noticeable improvements in deep sleep, energy, and body composition typically take 3 to 6 months of sustained therapy.
11. Key Takeaways
- Distinct Biological Targets: The debate of sermorelin vs nad+ hinges on your clinical goals. NAD+ optimizes the intracellular mitochondrial engine, while sermorelin optimizes systemic endocrine signaling.
- Synergy Over Substitution: The most advanced longevity protocols do not choose between them; they stack them. Providing the body with the energy to heal (NAD+) alongside the hormonal signal to heal (Sermorelin) yields compounded regenerative outcomes.
- Bioavailability is Paramount: NAD+ requires IV, SubQ, or precursor delivery to bypass first-pass liver metabolism, while sermorelin demands precise, nighttime subcutaneous injections to align with the body’s natural circadian hGH pulses.
- Laboratory Sourcing Standards: Both compounds are highly sensitive to thermal and oxidative degradation. B2B purchasers and clinical compounders must mandate third-party HPLC testing and maintain rigorous cold-chain protocols to ensure therapeutic efficacy.
- Targeted Longevity: Choose NAD+ to combat brain fog, chronic fatigue, and genomic instability. Choose sermorelin to reverse age-related muscle loss, optimize sleep architecture, and accelerate structural recovery.