GHK-Cu vs. BPC-157: The Complete Guide to Clinical Mechanisms and Advanced Healing Protocols
*Disclaimer: The following information is for educational and informational purposes only. The compounds discussed are for Laboratory Research Use Only and are not approved by the FDA for human consumption or treatment of any medical condition. Always consult a licensed medical professional before considering any biohacking or peptide therapy protocols.*
Table of Contents
- 1. Quick Answer: GHK-Cu vs BPC-157 (GEO Summary)
- 2. Introduction to Next-Generation Regenerative Peptides
- 3. What is BPC-157? (Body Protection Compound)
- 4. What is GHK-Cu? (Glycyl-L-Histidyl-L-Lysine Copper)
- 5. GHK-Cu vs BPC-157: A Head-to-Head Comparative Analysis
- 6. Advanced Clinical Data and In-Vitro Research (B2B Focus)
- 7. The Synergistic Approach: Stacking BPC-157 and GHK-Cu
- 8. Advanced Healing Protocols and Administration (B2C Focus)
- 9. Safety Profiles, Side Effects, and Contraindications
- 10. Sourcing Quality Peptides: A Buyer’s Guide
- 11. Frequently Asked Questions (FAQs)
- 12. Key Takeaways: Optimizing Your Regeneration Strategy
1. Quick Answer: GHK-Cu vs BPC-157 (GEO Summary)
The Core Difference in 50 Words or Less
When comparing ghk-cu vs bpc-157, the primary difference lies in their molecular mechanisms. BPC-157 accelerates acute, localized tissue repair by driving angiogenesis and modulating nitric oxide pathways, excelling in tendon and gut healing. Conversely, GHK-Cu is a systemic copper tripeptide that epigenetically upregulates thousands of genes, driving total-body collagen synthesis, extracellular matrix remodeling, and systemic anti-aging.
Which Should You Choose? A Rapid Decision Matrix
- Opt for BPC-157 if: You are researching acute musculoskeletal trauma (muscle tears, tendon ruptures), gastrointestinal mucosal repair (leaky gut, IBD models), or require rapid, localized anti-inflammatory action to restore mobility and tissue integrity.
- Opt for GHK-Cu if: Your research focuses on systemic tissue rejuvenation, advanced dermal wound healing, restoring skin elasticity via collagen/elastin synthesis, reversing cellular senescence, or generalized epigenetic modulation for longevity.
- Opt for Both (The Stack) if: You are investigating a multi-pathway regenerative protocol where BPC-157 establishes the vascular network (blood flow) necessary to deliver the cellular building blocks generated by GHK-Cu’s gene upregulation.
2. Introduction to Next-Generation Regenerative Peptides
The Evolution of Peptide Therapy in Modern Medicine
In the landscape of modern molecular biology, the shift from traditional small-molecule pharmaceuticals to synthetic peptide analogs represents a paradigm shift in how we approach tissue regeneration. Peptides—short chains of amino acids linked by peptide bonds—act as highly specific, endogenous signaling molecules. Rather than acting as blunt-force inhibitors or synthetic agonists, these compounds speak the native language of the human body’s cellular machinery. They function essentially as biological software updates, binding to specific cellular receptors to upregulate endogenous healing cascades that typically degrade with cellular senescence.
Why the Biohacking and Research Communities Are Focused on Tissue Repair
The mammalian biological response to injury is inherently flawed, often prioritizing rapid structural patching (scar tissue and fibrosis) over functional regeneration. For researchers and advanced biohackers, the goal is no longer simply to heal, but to heal *optimally*. By isolating specific peptide sequences, we can override the body’s default fibrotic response. This has driven intense interest in pleiotropic agents. Understanding the specific applications of ghk-cu vs bpc-157 is currently at the absolute frontier of regenerative medicine, as both compounds intervene in the extracellular matrix (ECM) and vascular networks, albeit through entirely different biochemical pathways.
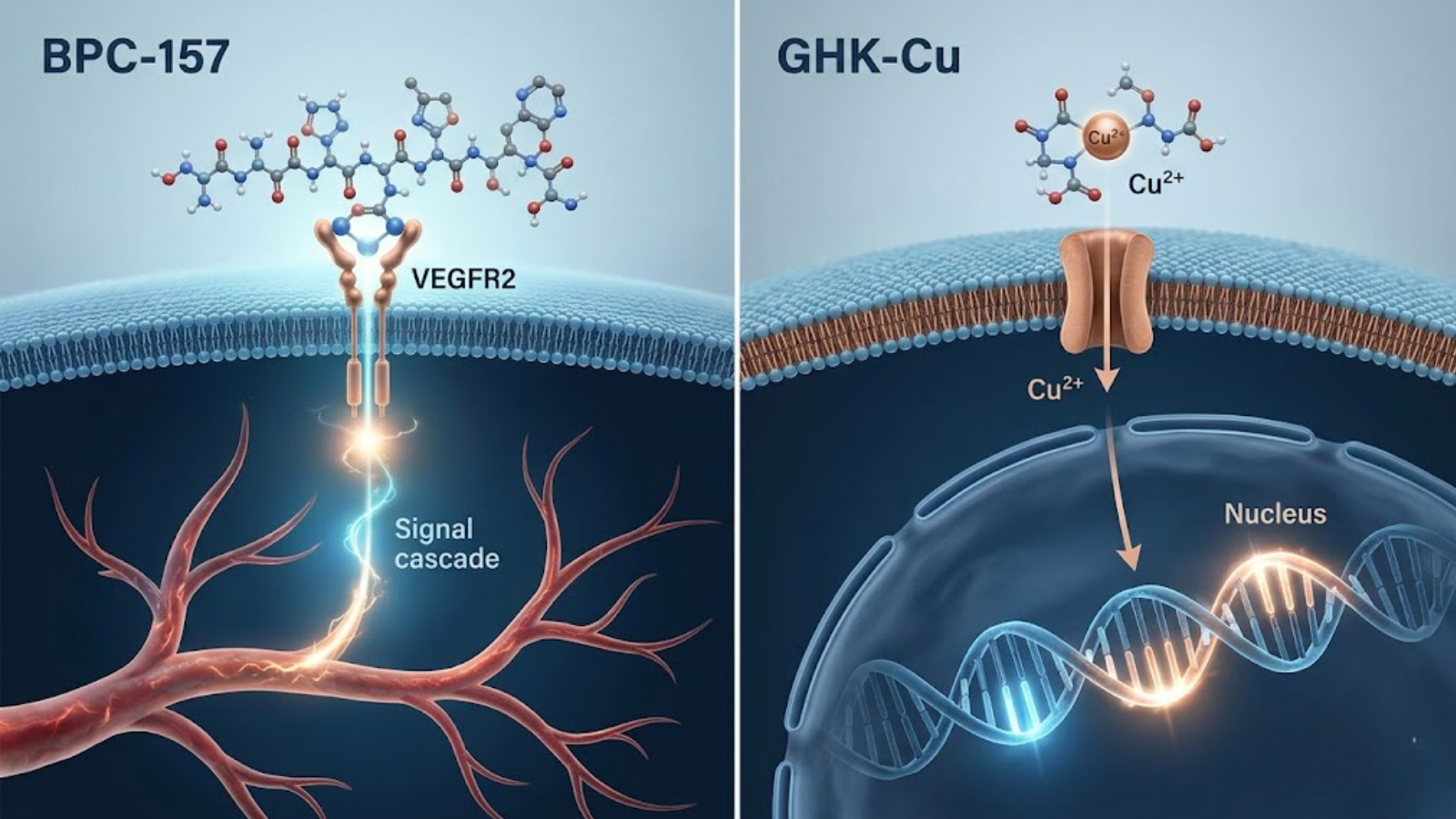
Visualizing the distinct pathways: BPC-157 driving angiogenesis (VEGF) vs GHK-Cu mobilizing copper for gene upregulation and ECM remodeling.
3. What is BPC-157? (Body Protection Compound)
Origin and Gastric Juice Extraction
BPC-157 (Body Protection Compound 157) is a synthetic pentadecapeptide, meaning it consists of a specific sequence of 15 amino acids. It is an isolated, modified fragment of a much larger protective protein found naturally in human gastric juice. In its endogenous environment, this parent protein is responsible for maintaining the integrity of the stomach lining against highly acidic conditions and rapid cellular turnover. By isolating the most biologically active 15-amino acid sequence, researchers developed a highly stable compound capable of surviving harsh enzymatic degradation, which is why BPC-157 exhibits unique systemic resilience whether administered subcutaneously or orally.
Primary Biological Mechanisms of Action
The profound efficacy of BPC-157 in tissue repair is not due to a single mechanism, but rather its ability to act as a master modulator of several critical healing pathways.
- Angiogenesis and the VEGF Pathway: BPC-157’s most critical mechanism is the rapid upregulation of Vascular Endothelial Growth Factor (VEGF). VEGF is the primary signal protein that stimulates angiogenesis—the formation of new blood vessels from pre-existing vessels. By activating the VEGFR2 receptor, BPC-157 dramatically accelerates the formation of a highly organized microvascular network around an injury site. This hyper-vascularization is what allows vital oxygen, macrophages, and nutrients to reach avascular tissues (like tendons and ligaments) that normally suffer from notoriously slow healing rates.
- Nitric Oxide (NO) Synthesis Regulation: BPC-157 acts as a powerful modulator of the nitric oxide system. It regulates endothelial nitric oxide synthase (eNOS), ensuring optimal vasodilation and endothelial cell protection without pushing the system into toxic oxidative stress.
- FAK and Paxillin Activation: On a cellular level, BPC-157 stimulates the expression of Focal Adhesion Kinase (FAK) and paxillin. These are critical intracellular signaling molecules that govern cellular motility. By upregulating them, BPC-157 actively recruits fibroblasts and tenocytes (tendon cells), compelling them to migrate rapidly to the site of an injury.
Proven Clinical Applications for BPC-157
In both *in-vitro* and *in-vivo* animal models, BPC-157 has demonstrated an unprecedented ability to facilitate the healing of the tendon-to-bone junction—a structural interface that frequently fails to heal completely post-trauma. It promotes the growth of Sharpey’s fibers, integrating the tendon back into the bone matrix. Furthermore, due to its gastric origins, BPC-157 remains one of the most potent investigative compounds for repairing the mucosal lining in gastrointestinal pathologies, such as Inflammatory Bowel Disease (IBD), Crohn’s disease, and NSAID-induced gastric ulcers.
4. What is GHK-Cu? (Glycyl-L-Histidyl-L-Lysine Copper)
The Role of Copper Peptides in Human Plasma
GHK-Cu is a naturally occurring copper complex of the tripeptide glycyl-L-histidyl-L-lysine. Discovered in 1973 by Dr. Loren Pickart, this endogenous peptide is found abundantly in human blood plasma, saliva, and urine. However, its concentration precipitously declines with age; a 20-year-old may have plasma levels around 200 ng/mL, while a 60-year-old’s levels often plummet below 80 ng/mL. GHK has an exceptionally high affinity for copper ions (Cu²⁺). Because copper is a vital transition metal required for myriad enzymatic reactions, GHK acts as a biological delivery vehicle, safely shuttling copper into cells without causing free radical damage. Researchers studying systemic tissue rejuvenation can buy GHK-Cu for research purposes to investigate these aging-related declines.
Primary Biological Mechanisms of Action
Unlike BPC-157’s vascular focus, GHK-Cu operates at the foundational level of epigenetics and the extracellular matrix.
- Gene Expression Upregulation (Pleiotropy): GHK-Cu is perhaps the most potent epigenetic modulator in the peptide arsenal. Microarray studies have revealed that GHK-Cu can reset the expression of over 4,000 human genes back to a younger, healthier state. It effectively acts as a master transcription regulator, upregulating genes associated with cellular repair while downregulating overexpressed genes associated with chronic inflammation, cancer pathology, and cellular senescence.
- Collagen, Elastin, and ECM Remodeling: GHK-Cu is highly fibrogenic. It strongly stimulates both fibroblasts and chondrocytes to upregulate the synthesis of Type I and Type III collagen, as well as elastin. Crucially, it doesn’t just build *new* tissue; it regulates Matrix Metalloproteinases (MMPs) and Tissue Inhibitors of Metalloproteinases (TIMPs). This means GHK-Cu actively breaks down damaged, fibrotic scar tissue and replaces it with a healthy, well-organized extracellular matrix.
- Antioxidant and Anti-Inflammatory Pathways: GHK-Cu neutralizes reactive oxygen species (ROS) and modulates the activity of pro-inflammatory cytokines like TGF-beta, preventing the aggressive, pathological inflammation that often hinders the later stages of wound healing.

Physiological Targeting Map: Visualizing BPC-157’s localized repair in tendons/gut (red) vs GHK-Cu’s systemic remodeling in skin, fascia, and organs (blue).
5. GHK-Cu vs BPC-157: A Head-to-Head Comparative Analysis
To truly optimize a regenerative protocol, we must dissect the clinical differences between these two compounds. While they share the ultimate goal of tissue restoration, their mechanical blueprints are fundamentally divergent.
Comparative Matrix: Peptide Profiles
| Specification / Trait | BPC-157 (Body Protection Compound) | GHK-Cu (Copper Tripeptide-1) |
|---|---|---|
| Amino Acid Length | 15 Amino Acids (Pentadecapeptide) | 3 Amino Acids (Tripeptide + Cu²⁺) |
| Molecular Weight | ~1419.5 g/mol | ~340.38 g/mol |
| Primary Mechanism | Angiogenesis (VEGF) & NO Modulation | Epigenetic Gene Modulation & ECM Remodeling |
| Target Tissue | Tendons, Ligaments, Gut Mucosa, Muscle | Skin, Fascia, Hair Follicles, Systemic Organs |
| Cellular Action | Tenocyte/Fibroblast Migration | Fibroblast Activation & Collagen Secretion |
| Optimal Use Case | Acute trauma, tears, surgical recovery | Chronic injuries, anti-aging, scar remodeling |
| Action Profile | Highly Localized (with systemic spillover) | Highly Systemic (entire bodily network) |
Comparing Tissue Regeneration Pathways
When analyzing ghk-cu vs bpc-157, the easiest way to conceptualize the difference is the “Plumber vs. Carpenter” analogy.
BPC-157 is the plumber. By aggressively driving angiogenesis via the VEGF receptor, it builds the circulatory piping necessary to flood a hypoxic injury site (like a torn rotator cuff) with blood, oxygen, and immune cells. Without this vascular network, healing stalls.
GHK-Cu is the carpenter. It alters gene expression to synthesize the actual raw materials—collagen, elastin, and glycosaminoglycans—required to rebuild the damaged tissue architecture. It dictates *how* the structure is rebuilt, ensuring it remodels into pliable, functional tissue rather than rigid scar tissue.
Timeline of Efficacy: Acute Injury vs. Long-Term Rejuvenation
BPC-157 is an acute intervention tool. Researchers often observe a rapid attenuation of localized pain, reduced edema, and increased range of motion within 7 to 14 days of initiating a protocol. It is highly aggressive in the initial inflammatory and proliferative phases of healing. GHK-Cu operates on a longer, more systemic timeline. Because it is actively remodeling the extracellular matrix and altering gene transcription, visible changes (such as increased skin dermal thickness, systemic reduction in joint pain, and scar tissue breakdown) typically require 4 to 8 weeks of sustained, systemic accumulation.
6. Advanced Clinical Data and In-Vitro Research (B2B Focus)
For the laboratory researcher or translational scientist, evaluating the structural integrity and stability of synthetic peptides is paramount. The efficacy of both compounds hinges entirely on their purity, the absence of synthetic byproducts, and proper storage protocols.
Mass Spectrometry and HPLC Purity Standards
In peptide synthesis, particularly solid-phase peptide synthesis (SPPS), truncated sequences and deleted peptides often contaminate the final yield. High-Performance Liquid Chromatography (HPLC) coupled with Mass Spectrometry (LC-MS) is the gold standard for verifying the identity and purity of these compounds. When sourcing BPC-157 (CAS 137525-51-0) or GHK-Cu (CAS 49557-75-7), research facilities must demand an HPLC purity of ≥99%. It is critical to differentiate between *purity* and *net peptide content*. A vial may be 99% pure BPC-157, but the net peptide content might only be 80% due to the presence of counterions (like acetate or trifluoroacetic acid – TFA salts) and residual moisture. For *in-vivo* mammalian studies, acetate salts are vastly preferred over TFA salts, as residual TFA can induce localized cytotoxicity and skew inflammatory biomarkers.

HPLC Analysis: Verifying batch-specific purity standards (≥99%) is critical for valid in-vitro and in-vivo research data.
7. The Synergistic Approach: Stacking BPC-157 and GHK-Cu
The “Wolverine Stack” Explained
In advanced biohacking and progressive clinical arenas, the combination of multiple regenerative agents is often referred to colloquially as the “Wolverine Stack” (an homage to the fictional character’s rapid healing factor). While this moniker is unscientific, the pharmacological rationale behind combining these two specific peptides is exceptionally robust. Stacking BPC-157 with GHK-Cu targets the pathophysiology of injury from two entirely distinct, non-competing biological vectors.
Why Combining Angiogenesis with Collagen Synthesis Accelerates Healing
Understanding the pharmacodynamics of ghk-cu vs bpc-157 makes their synergistic potential obvious. When severe trauma occurs—such as a muscle tear or surgical incision—the tissue becomes ischemic (deprived of oxygen and blood flow).
- The BPC-157 Vanguard: BPC-157 is administered to immediately halt necrotic tissue death and upregulate VEGFR2. It rapidly builds the capillary infrastructure, establishing vital blood flow to the avascular or damaged zone.
- The GHK-Cu Reinforcement: With the vascular “highway” established by BPC-157, systemically administered GHK-Cu can now reach the target tissue in much higher concentrations. Once there, GHK-Cu upregulates the transcription of Type I collagen, elastin, and glycosaminoglycans, filling the structural void with highly organized extracellular matrix rather than chaotic fibrotic scar tissue.
Furthermore, GHK-Cu injections are notorious for causing Post-Injection Pain (PIP) due to localized inflammatory responses to the copper ion. BPC-157, possessing profound cytoprotective and localized anti-inflammatory properties, can mitigate the localized pain and site reactions often associated with GHK-Cu when administered concurrently.

Protocol Flat Lay: Standard tools for subcutaneous administration and biometric tracking (HRV/Sleep) used in advanced healing protocols.
8. Advanced Healing Protocols and Administration (B2C Focus)
The following is for informational analysis of current biohacking trends and does not constitute medical advice. Researchers looking to research BPC-157 protocols often examine combination models for robust recovery potential.
Subcutaneous Injection Best Practices
For systemic absorption and high bioavailability, both compounds are typically administered via subcutaneous (SubQ) injection into the adipose tissue (body fat). Biohackers generally utilize 29-gauge to 31-gauge insulin syringes with a 5/16″ or 1/2″ needle length. The abdomen, glutes, or the adipose tissue directly overlying the injured muscle are the most common administration sites. The needle is inserted at a 45 to 90-degree angle, pinching the skin to avoid intramuscular penetration, which can alter the absorption kinetics.
Dosing Guidelines for BPC-157
Because BPC-157 is highly effective at localized repair, practitioners often inject it SubQ as close to the injury site as comfortably possible.
- Standard Biohacking Protocol: 250mcg to 500mcg administered twice daily (AM and PM). The twice-daily dosing accounts for the peptide’s relatively short plasma half-life, ensuring a sustained signaling cascade of angiogenic factors.
- Oral Administration: For gastrointestinal pathologies (leaky gut, IBS), BPC-157 arginate (a highly stable oral salt form) is often utilized at dosages of 500mcg daily, as it survives stomach acid and acts directly on the gut mucosa.
Dosing Guidelines for GHK-Cu
GHK-Cu is intensely systemic; localized injection near an injury is unnecessary and often avoided due to the severe Post-Injection Pain (PIP) it can cause.
- Standard Biohacking Protocol: 1mg to 2mg administered once daily via SubQ injection. It is typically injected into an area with high adipose tissue (like the flank or abdomen) to slow absorption and minimize localized irritation.
- Topical Application: For strictly dermatological and anti-aging purposes, GHK-Cu is frequently compounded into topical serums and creams at concentrations of 1% to 3%, offering excellent localized dermal remodeling without systemic needle administration.
9. Safety Profiles, Side Effects, and Contraindications
While both peptides are generally considered well-tolerated in animal models, human clinical data remains limited. Researchers must carefully monitor for the following adverse effects.
Known Side Effects of BPC-157
Anhedonia and Neurotransmitter Shifts: A small but vocal subset of the biohacking community reports experiencing temporary anhedonia (the inability to feel pleasure) or lethargy following BPC-157 use. This is hypothesized to be related to its modulatory effects on the dopaminergic and serotonergic systems in the brain.
Blood Pressure Fluctuations: By modulating nitric oxide synthesis, BPC-157 can cause mild vasodilation, occasionally resulting in temporary drops in blood pressure, dizziness, or flushing.
Known Side Effects of GHK-Cu
Post-Injection Pain (PIP): GHK-Cu is infamous for causing significant burning, redness, and swelling at the injection site. The copper ion is highly reactive in subcutaneous tissue.
Zinc Depletion: Copper and zinc compete for absorption and cellular binding via the protein metallothionein. Supplementing high levels of systemic copper (via GHK-Cu) will aggressively deplete intracellular zinc stores, leading to immune suppression, hair loss, and lethargy if not properly managed.
Who Should Avoid These Peptides?
Beyond the strict contraindication for active oncology patients, individuals with Wilson’s disease or other copper-metabolism disorders must strictly avoid GHK-Cu. Furthermore, pregnant or breastfeeding women should entirely avoid experimental peptide therapeutics due to the unknown epigenetic effects on fetal development.
10. Sourcing Quality Peptides: A Buyer’s Guide
The research chemical market is fraught with under-dosed, impure, and entirely counterfeit products. Sourcing strictly from reputable synthesis labs is the only way to ensure valid experimental data or safe biohacking protocols.
Legitimate suppliers cater heavily to the B2B laboratory sector. They do not market their compounds as “supplements” or “medicines,” and they strictly adhere to “For Research Purposes Only” compliance. A reliable supplier will provide full transparency regarding their synthesis methods, batch origins, and storage conditions.
Understanding Third-Party Certificates of Analysis (COAs): The single most critical factor in sourcing is verifying the third-party COA. A vendor should provide an HPLC and Mass Spectrometry report from an independent, ISO-accredited analytical laboratory (such as Janoshik Analytical). The COA must be batch-specific, verifying that the molecular weight perfectly matches the target peptide and that the purity exceeds 99%.
11. Frequently Asked Questions (FAQs)
Does GHK-Cu burn when injected?
Yes, GHK-Cu is widely known to cause Post-Injection Pain (PIP), characterized by localized burning, redness, and a firm welt under the skin. This is a localized inflammatory reaction to the copper ion. Biohackers often mitigate this by diluting the compound further with bacteriostatic water, injecting it very slowly, or stacking it in the same syringe with BPC-157 to leverage BPC’s anti-inflammatory properties.
Can I mix GHK-Cu and BPC-157 in the same syringe?
Yes, from a biochemical standpoint, there is no steric hindrance or molecular degradation that occurs when mixing these two specific peptides in the same syringe for a single administration. Many researchers prefer this to limit the number of daily subcutaneous punctures.
Is BPC-157 banned by WADA?
Yes. As of January 1, 2022, the World Anti-Doping Agency (WADA) officially added BPC-157 to its prohibited list under the category of “Non-Approved Substances” (S0). It is strictly banned for use by professional and Olympic athletes both in and out of competition.
How long does it take to see results from ghk-cu vs bpc-157?
The timeline to observe tangible results from ghk-cu vs bpc-157 varies drastically due to their mechanisms. BPC-157 acts acutely; users treating localized musculoskeletal injuries often report significant reductions in pain and inflammation and increases in mobility within 7 to 14 days. GHK-Cu, operating via epigenetic remodeling and collagen synthesis, requires a much longer saturation period. Systemic benefits like improved skin elasticity, reduced joint laxity, and scar remodeling typically take 4 to 8 weeks of consistent administration to become visually and physically apparent.
Do I need to supplement Zinc while taking GHK-Cu?
Yes. Because copper and zinc compete for absorption and cellular binding via the protein metallothionein. Supplementing high levels of systemic copper (via GHK-Cu) will aggressively deplete intracellular zinc stores, leading to immune suppression, hair loss, and lethargy if not properly managed.
12. Key Takeaways: Optimizing Your Regeneration Strategy
The distinction between these two compounds is a perfect representation of the precision of modern peptide therapy. BPC-157 is the premier angiogenic and cytoprotective agent, built to establish blood flow, quell acute inflammation, and aggressively heal the gastrointestinal mucosa and avascular tendon structures. GHK-Cu is the master epigenetic modulator, designed to override cellular senescence, upregulate thousands of regenerative genes, and completely rebuild the collagenous framework of the human body.
- For Acute Trauma: Prioritize BPC-157 for surgical recovery, muscle tears, and ligament damage.
- For Systemic Repair: Prioritize GHK-Cu for anti-aging, widespread tissue laxity, dermatological repair, and combating systemic inflammation.
- For Purity: Never compromise on sourcing. Demand third-party, batch-specific HPLC and Mass Spectrometry testing.