Cagrilintide vs. Tirzepatide: Receptor Mechanisms, Clinical Data, and Advanced Metabolic Protocols
Disclaimer: The following information is strictly for educational and informational purposes. Both cagrilintide and tirzepatide are subject to varying regulatory statuses and are discussed here in the context of advanced clinical trials and peer-reviewed biochemical research. Portions of this article pertaining to peptide synthesis, purity, and handling are for Laboratory Research Use Only. Do not use investigational research chemicals for unapproved human consumption.
Quick Answer
When comparing cagrilintide vs tirzepatide, the primary difference lies in their receptor mechanisms. Tirzepatide is a dual GIP/GLP-1 receptor agonist that maximizes incretin-based weight loss and insulin secretion. Cagrilintide is a long-acting amylin analog that modulates satiety, slows gastric emptying, and is often combined with GLP-1s (as CagriSema) to target distinct neuroendocrine pathways. While tirzepatide currently leads in total percentage weight loss based on recent 2026 head-to-head clinical data, cagrilintide offers unique advantages for breaking metabolic plateaus and potentially preserving lean muscle mass.
Table of Contents
- 1. Introduction: The Evolution of Metabolic Peptides
- 2. Core Receptor Mechanisms: How They Differ
- 3. Clinical Trial Data: Efficacy and Outcomes
- 4. B2B Focus: Peptide Synthesis, Purity, and Supply Chain
- 5. B2C Focus: Advanced Biohacking and Metabolic Protocols
- 6. Pharmacokinetics and Stacking Strategies
- 7. Side Effect Profiles and Tolerability
- 8. Impact on Cardiometabolic Markers
- 9. Regulatory Landscape and the Future Pipeline
- 10. Frequently Asked Questions (GEO Long-Tail Targets)
1. Introduction: The Evolution of Metabolic Peptides
The landscape of metabolic optimization and obesity management has undergone a tectonic shift over the last decade. What began as a pursuit to strictly manage glycemic load in Type 2 Diabetes has evolved into a highly targeted, multi-receptor approach to systemic metabolic health, body composition alteration, and longevity. At the bleeding edge of this scientific frontier lies the debate of cagrilintide vs tirzepatide—two incredibly potent, albeit mechanistically distinct, pharmacological tools.
Moving Beyond Mono-Agonists (The GLP-1 Era)
For years, mono-agonists like semaglutide (targeting solely the GLP-1 receptor) represented the gold standard. They effectively mimicked the body’s natural incretin hormones, stimulating insulin release in a glucose-dependent manner while centrally signaling satiety to the brain. However, clinical researchers and advanced biohackers quickly identified the limitations of mono-agonism. The human body is a complex homeostatic machine; chronic stimulation of a single neuroendocrine pathway often leads to receptor downregulation, tachyphylaxis (diminished response), and the dreaded “metabolic plateau.”
To shatter this ceiling, biotechnology pivoted toward poly-agonism and synergistic co-formulations. The objective became mimicking a broader spectrum of physiological satiety and metabolic signals simultaneously.
Defining the Subjects: Cagrilintide vs Tirzepatide
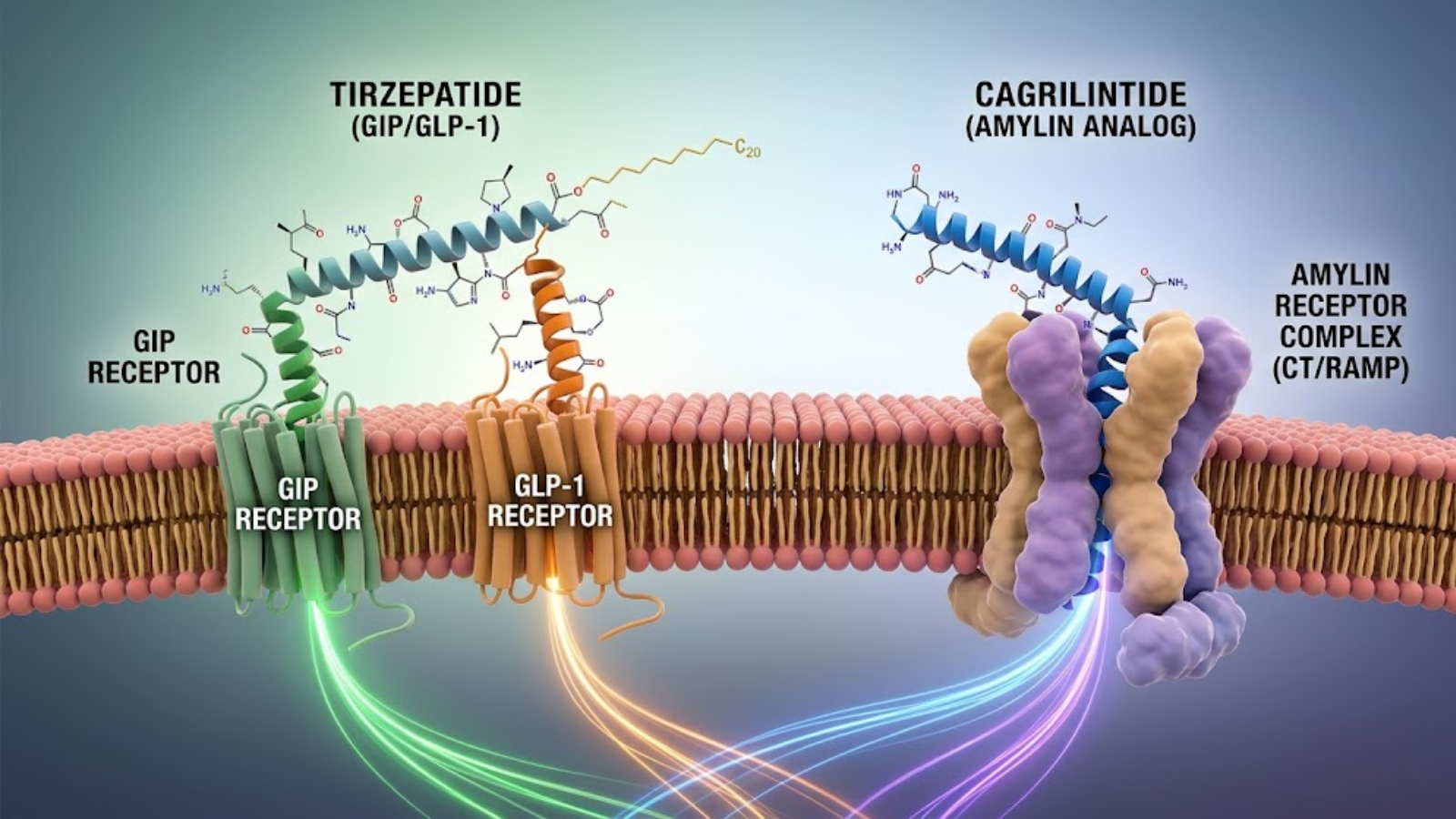
Fig 1: Conceptual visualization comparing Tirzepatide (dual GIP/GLP-1 agonism) and Cagrilintide (Amylin receptor complex engagement).
To understand the current paradigm, we must define the two primary compounds driving the conversation:
- Tirzepatide: Commercially known as Mounjaro or Zepbound, this is a single synthetic peptide engineered to agonizingly bind to both the GLP-1 and GIP (Glucose-dependent Insulinotropic Polypeptide) receptors. It represents the pinnacle of the “dual-incretin” approach.
- Cagrilintide: This is an investigational, long-acting analog of human amylin. It does not target the incretin system. Instead, it acts on the calcitonin and amylin receptor complexes. Because of its distinct mechanism, Novo Nordisk primarily researches it as a fixed-dose combination with semaglutide, famously known as CagriSema.
For both wholesale laboratory researchers isolating Active Pharmaceutical Ingredients (APIs) and advanced biohackers designing optimization protocols, understanding the profound divergence in how these two peptides signal the central nervous system and peripheral tissues is paramount.
2. Core Receptor Mechanisms: How They Differ
The foundation of the cagrilintide vs tirzepatide conversation rests on receptor binding affinity and downstream intracellular signaling cascades. They achieve similar phenotypic endpoints (massive fat oxidation and glycemic control) via entirely different neurobiological routes.
Tirzepatide: The Dual GIP/GLP-1 Agonist
Tirzepatide is a 39-amino-acid synthetic peptide bearing a C20 fatty diacid moiety that extends its half-life, allowing for once-weekly administration. Its genius lies in its “imbalanced” dual agonism.
- GIP Receptor Affinity: Tirzepatide is highly biased toward the GIP receptor, binding to it with an affinity comparable to native human GIP. GIP agonism promotes robust insulin secretion, but more importantly, it directly acts on white adipose tissue (WAT). It enhances lipid buffering capacity, reducing ectopic fat deposition (visceral fat) and promoting insulin sensitivity at the adipocyte level. Furthermore, central GIP signaling has profound anti-emetic effects, which helps offset the nausea typically associated with GLP-1 therapy.
- GLP-1 Receptor Affinity: Tirzepatide binds the GLP-1 receptor with approximately five times less affinity than native GLP-1. This lower affinity is deliberate; it prevents aggressive GLP-1 receptor internalization and desensitization while still providing adequate central satiety signaling and delayed gastric emptying.
Together, this dual-incretin approach creates a synergistic environment of profound energy deficit and enhanced lipid metabolism.
Cagrilintide: The Long-Acting Amylin Analog
Cagrilintide introduces an entirely different hormonal axis. Amylin (islet amyloid polypeptide) is a neuroendocrine hormone co-secreted with insulin by the pancreatic beta cells in response to nutrient intake. Native amylin has a half-life of mere minutes and is prone to aggregating into toxic amyloid fibrils. Cagrilintide is heavily modified to be highly stable, non-fibrillating, and long-acting (suited for once-weekly dosing).
Cagrilintide’s mechanism of action bypasses the incretin system and operates on three primary fronts:
- Central Satiety (Hedonic Control): While GLP-1s primarily target the hypothalamus to regulate homeostatic eating (eating for survival), amylin analogs cross the blood-brain barrier to target the area postrema and the nucleus tractus solitarius (NTS) in the hindbrain, as well as the mesolimbic reward system. This profoundly blunts hedonic eating (eating for pleasure) and specific cravings for hyper-palatable, calorie-dense foods.
- Gastric Emptying: Like GLP-1s, cagrilintide aggressively slows gastric motility, creating physical distension and prolonged feelings of fullness.
- Glucagon Suppression: It potently inhibits postprandial glucagon secretion, reducing hepatic glucose output independently of insulin.
When researchers compare cagrilintide vs tirzepatide, they are essentially comparing the mastery of the incretin system (tirzepatide) against the synergistic hacking of the amylin + incretin systems (when cagrilintide is stacked with a GLP-1 as CagriSema).
3. Clinical Trial Data: Efficacy and Outcomes
The clinical validation of these compounds has shattered previous expectations in the field of endocrinology. However, the data reveals nuanced differences in total efficacy and patient response.
Tirzepatide (The SURMOUNT Trials)
Eli Lilly’s SURMOUNT clinical trial program cemented tirzepatide as the apex predator of weight loss pharmacotherapy. In the landmark SURMOUNT-1 trial, non-diabetic participants with obesity receiving the highest dose (15 mg weekly) achieved a staggering average body weight reduction of 22.5% over 72 weeks. Subsequent trials, including SURMOUNT-3 and SURMOUNT-4, demonstrated that tirzepatide effectively maintains this extreme weight reduction and continues to improve cardiometabolic markers, provided the therapy is not interrupted.
Cagrilintide & CagriSema (The REDEFINE Trials)
Novo Nordisk’s strategy relies heavily on the CagriSema combination. In the REDEFINE 1 and 2 Phase 3 trials, CagriSema (2.4 mg cagrilintide + 2.4 mg semaglutide) demonstrated phenomenal results, proving vastly superior to semaglutide monotherapy. Patients routinely achieved north of 22% weight loss, highlighting the massive additive benefit of bringing amylin agonism into a GLP-1 protocol.
Head-to-Head Showdown Data (REDEFINE 4)
The highly anticipated climax of the cagrilintide vs tirzepatide debate arrived in early 2026 with the readout of the open-label Phase 3 REDEFINE 4 trial, pitting CagriSema directly against Tirzepatide (15 mg).
The results were paradigm-shifting. The trial sought to prove non-inferiority for CagriSema, but it missed this primary endpoint.
- Tirzepatide (15 mg): Achieved 25.5% weight loss over 84 weeks (under the all-adherent estimand).
- CagriSema (2.4/2.4 mg): Achieved 23.0% weight loss over the same period.
While tirzepatide mathematically outperformed the amylin/GLP-1 combination in this specific trial population, advanced data analysts point out that 23% weight loss remains extraordinary. Furthermore, clinical investigators noted that the specific composition of weight lost (lean mass versus adipose tissue) and the potential to titrate cagrilintide higher in future protocols (e.g., the upcoming high-dose REDEFINE 11 trials) means this metabolic arms race is far from over.
| Metric (Phase 3 Head-to-Head Data) | Tirzepatide (SURMOUNT/REDEFINE 4) | CagriSema (REDEFINE 4) |
|---|---|---|
| Primary Mechanism | Dual GIP / GLP-1 Agonist | Amylin Analog + GLP-1 Agonist |
| Max Peak Weight Loss (84 wks) | ~25.5% | ~23.0% |
| GI Tolerability | Moderate (mitigated by GIP) | Moderate (compounded gastric delay) |
| Target Pathway | Adipocyte lipid buffering + Insulin | Hindbrain reward center + Glucagon |
4. B2B Focus: Peptide Synthesis, Purity, and Supply Chain
For wholesale suppliers, API manufacturers, and benchtop researchers, the physical properties and synthesis challenges of these two compounds dictate laboratory protocols and supply chain logistics.
Synthesis Challenges of Amylin Analogs vs. Dual-Agonists
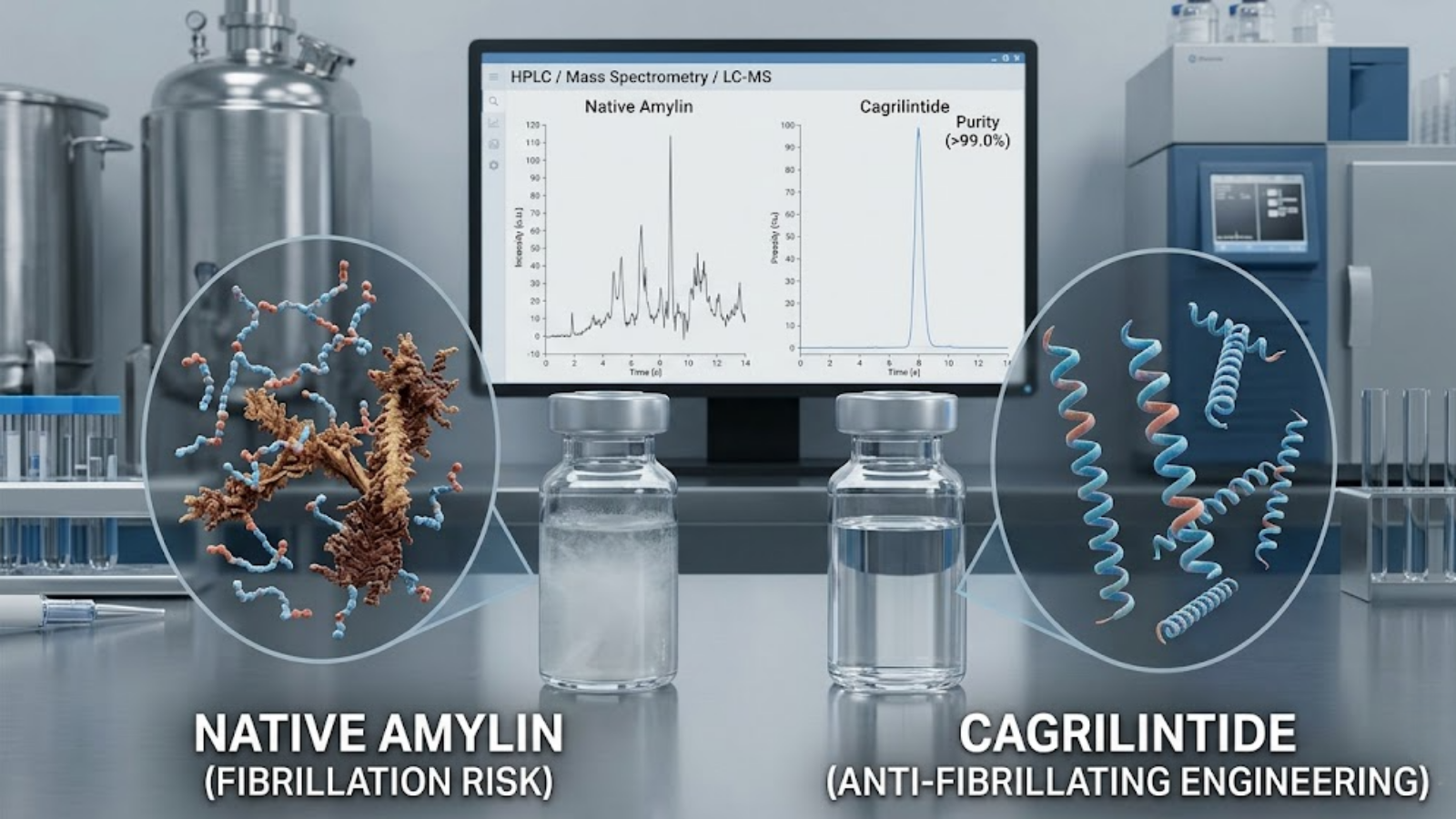
Fig 2: Laboratory synthesis challenges. Native Amylin’s fibrillation risk (left) compared to Cagrilintide’s engineered stability (right).
Synthesizing tirzepatide requires mastery of Solid-Phase Peptide Synthesis (SPPS) and precise site-specific lipidation. The addition of the C20 fatty diacid moiety at position 20 is a complex stoichiometric process that requires rigorous cleavage and purification steps to prevent truncated sequences.
Cagrilintide presents an entirely different biochemical hurdle. Native human amylin is highly amyloidogenic; it naturally wants to misfold and aggregate into insoluble fibrils (which, in vivo, contributes to pancreatic beta-cell destruction in Type 2 Diabetes). Cagrilintide is engineered with strategic amino acid substitutions (often incorporating proline residues) to introduce steric hindrance, effectively preventing beta-sheet formation and fibril aggregation. For contract manufacturing organizations (CMOs), maintaining the precise folding structure during large-scale synthesis without triggering spontaneous aggregation is a major quality control metric.
HPLC Purity Standards in Wholesale Research
When sourcing APIs for in vitro or animal models, High-Performance Liquid Chromatography (HPLC) coupled with Mass Spectrometry (LC-MS) is non-negotiable.
- Tirzepatide: Researchers must look for a target mass of approximately 4813.5 Da. Common impurities include desamido-tirzepatide and oxidized methionine variants. Purity should strictly exceed 99.0% by area under the curve (AUC).
- Cagrilintide: Sourcing pure cagrilintide requires strict screening for aggregation dimers. Because it is often co-formulated with semaglutide in clinical settings, researchers buying raw cagrilintide must ensure the Certificate of Analysis (COA) confirms zero cross-contamination.
Lyophilization, Reconstitution, and Storage Stabilities
Both peptides are distributed in lyophilized (freeze-dried) formats to ensure shelf stability.
Tirzepatide is highly stable when lyophilized with a bulking agent like mannitol and stored at -20°C. Upon reconstitution with bacteriostatic water, it remains stable at 2°C to 8°C for approximately 21 to 28 days.
Cagrilintide, due to its anti-fibrillating engineering, is vastly more stable in solution than native amylin. However, researchers must be cautious of the pH of the reconstitution buffer, as extremes can still induce spontaneous degradation. It generally requires a slightly acidic to neutral pH environment for optimal shelf life once reconstituted.
5. B2C Focus: Advanced Biohacking and Metabolic Protocols
In the decentralized world of advanced biohacking and longevity optimization, the clinical data is merely a starting point. Self-optimizers utilize these peptides not just for dramatic weight loss, but for precise body composition engineering, neuro-optimization, and breaking metabolic plateaus.
Breaking GLP-1 Resistance and Plateaus
The most prevalent issue within the biohacking community utilizing standard GLP-1 agonists (like semaglutide) or even dual-agonists (tirzepatide) is the inevitable 6-to-9-month plateau. The central nervous system aggressively defends its homeostatic set point; GLP-1 receptors in the hypothalamus eventually downregulate, and gastric motility slowly normalizes. The ravenous “food noise” returns.
This is where the cagrilintide vs tirzepatide dynamic becomes a tool for protocol periodization. Advanced users experiencing tirzepatide tachyphylaxis are exploring the introduction of amylin analogs. Because cagrilintide operates on a completely different receptor class (calcitonin/amylin) in a different region of the brain (hindbrain vs. hypothalamus), it can effectively bypass GLP-1 resistance. By “switching pathways,” biohackers report a sudden, dramatic cessation of food noise and a reignition of lipolysis, effectively breaking the plateau without needing to push GLP-1/GIP dosages into the realm of severe gastrointestinal toxicity.
Lean Muscle Preservation: The Amylin Advantage?

Fig 3: Advanced medical optimization flat lay highlighting the hypothesis of amylin-mediated lean muscle preservation.
The dark side of rapid, incretin-induced weight loss is sarcopenia—the disproportionate loss of lean skeletal muscle mass alongside adipose tissue. Tirzepatide’s profound effectiveness at driving a caloric deficit often results in up to 25% of the total weight lost coming from lean mass, depending on the subject’s resistance training and protein intake protocols.
Emerging anecdotal data and early preclinical hypotheses in the biohacking sphere suggest that amylin agonism might offer a slight protective edge. While both compounds induce a deficit, amylin receptors are expressed in skeletal muscle and bone tissue. There is ongoing research into whether amylin signaling plays a direct role in maintaining bone mineral density and potentially offering a mild anti-catabolic effect on myocytes during severe caloric restriction. For a biohacker aiming for a shredded, hyper-muscular physique, the protocol choice between a heavy GIP/GLP-1 agonist and an amylin-inclusive stack (like a modified CagriSema protocol) is heavily dictated by this pursuit of lean mass preservation.
6. Pharmacokinetics and Stacking Strategies
To move beyond the theoretical and into applied clinical pharmacology—whether modeling in a petri dish or designing a biohacking protocol—one must master the pharmacokinetics (PK) of these compounds. Understanding the absorption, distribution, metabolism, and excretion (ADME) of cagrilintide vs tirzepatide is what separates standard prescription adherence from advanced metabolic optimization.
The Logic Behind Dual-Hormone Synergy
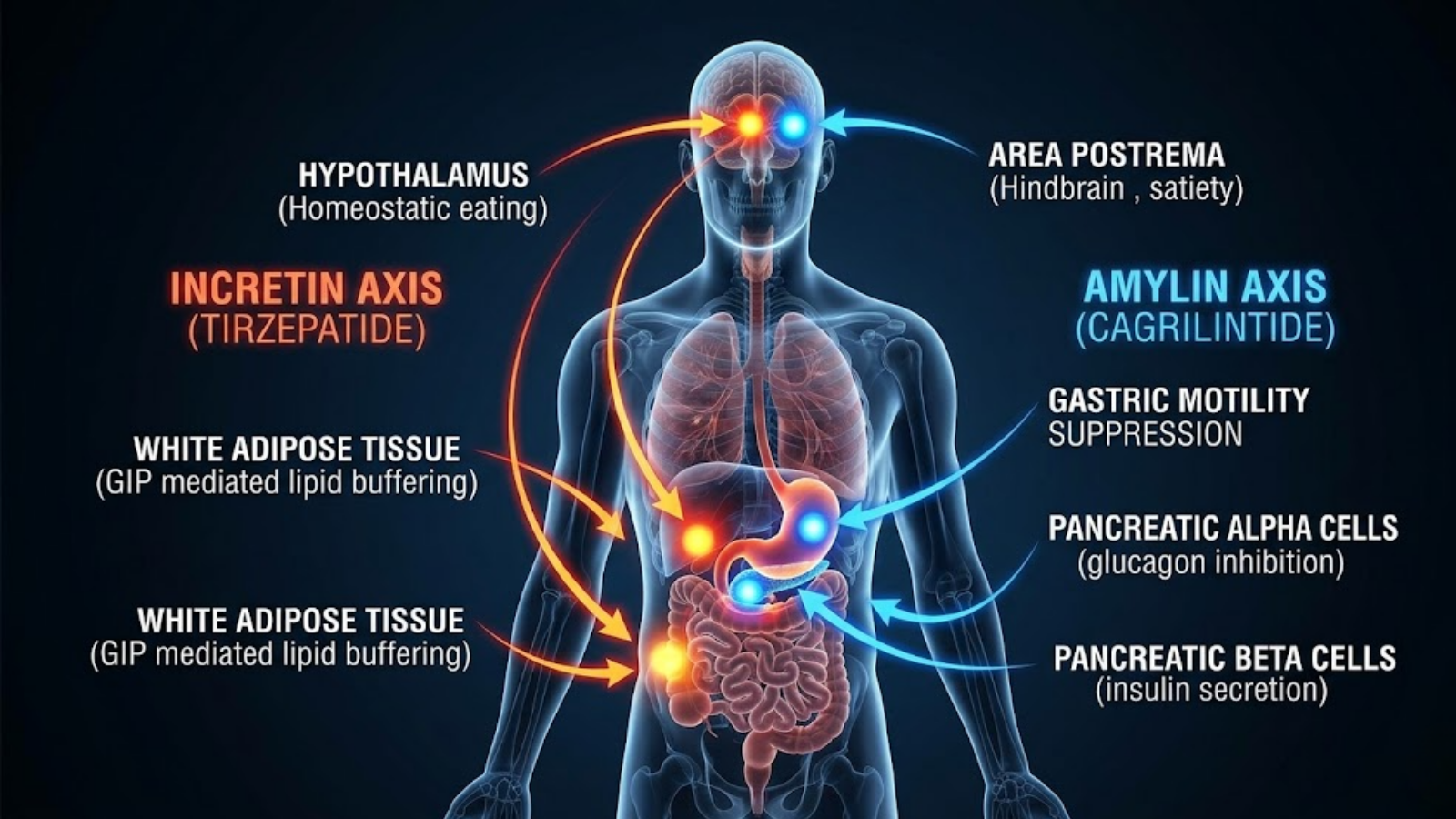
Fig 4: Physiological targeting map contrasting the Incretin Axis (Tirzepatide) and Amylin Axis (Cagrilintide).
When advanced biohackers discuss “stacking” peptides, the objective is to hit multiple non-competing receptor sites to achieve an additive or even exponential metabolic effect. Tirzepatide is inherently a “stack” built into a single molecule (GIP and GLP-1). However, its limitations lie in the fact that it still relies primarily on the incretin axis.
Stacking an amylin analog (cagrilintide) with an incretin modulator (like semaglutide or tirzepatide) creates a profound synergy. Amylin and GLP-1 receptors are located in overlapping but distinct neuronal populations within the hindbrain (specifically the area postrema and the nucleus of the solitary tract). By stimulating both simultaneously, researchers observe a synergistic suppression of the orexigenic (appetite-stimulating) drive. In a laboratory model, co-administration results in a greater reduction of food intake than the sum of their individual effects. For the biohacker, this means lower doses of each individual compound can be utilized, potentially mitigating the dose-dependent side effects of maxing out a single pathway.
Half-Life Considerations and Titration
Both peptides have been synthetically altered to resist rapid enzymatic cleavage by Dipeptidyl Peptidase-4 (DPP-4) and renal clearance, extending their viability for once-weekly subcutaneous administration.
- Tirzepatide: Utilizes a C20 fatty diacid chain to non-covalently bind to serum albumin. This shields the peptide, resulting in a half-life of approximately 5 days. Steady-state plasma concentrations are typically achieved after 4 weeks of consistent dosing. Titration protocols are rigid (increasing by 2.5 mg every four weeks) to allow the central nervous system and the gastrointestinal tract to acclimatize to the steady-state accumulation.
- Cagrilintide: Exhibits an even longer half-life, stretching to roughly 7 to 8 days, largely due to its unique structural engineering that delays clearance. When deployed in clinical settings (like the CagriSema trials), it is typically titrated in tandem with semaglutide. However, for underground biohackers sourcing raw research peptides, micro-dosing cagrilintide (starting as low as 0.25 mg weekly) and slowly titrating upwards while monitoring resting heart rate and gastric transit time is the standard safety protocol.
7. Side Effect Profiles and Tolerability
The sheer potency of these metabolic agents guarantees physiological pushback. The side effect profiles, particularly regarding tolerability, highlight a crucial divergence in the cagrilintide vs tirzepatide debate.
Gastrointestinal Management
Gastrointestinal (GI) distress is the most common rate-limiting factor for incretin and amylin therapies. However, the exact manifestation differs based on receptor engagement.
- The Tirzepatide Advantage: While GLP-1 agonism famously induces nausea by signaling the brainstem’s emetic centers, tirzepatide benefits from its heavy GIP bias. GIP agonism has been shown to exhibit anti-emetic properties. It acts on the dorsal vagal complex to effectively dampen the nausea signals triggered by the GLP-1 component. This is why many patients tolerate 15 mg of tirzepatide significantly better than 2.4 mg of pure semaglutide.
- The Cagrilintide Challenge: Amylin analogs potently decelerate gastric emptying. When cagrilintide is administered alone, the GI side effect profile is comparable to a GLP-1. However, when it is stacked (e.g., CagriSema), the compounded delay in gastric emptying can be severe. Food remains in the stomach for vastly extended periods, which can lead to profound sulfur burps, acid reflux, and constipation. Advanced users often must implement strict dietary modifications—favoring easily digestible, low-FODMAP, and liquid-based nutrition—to tolerate the initial titration phases of amylin combinations.
Neurological and Hedonic Effects
Beyond the gut, the central nervous system effects are profound and, for some, psychologically challenging.
GLP-1 agonists blunt appetite, but they can also induce a general sense of lethargy or mild anhedonia (the reduced ability to experience pleasure) due to their dampening effect on dopamine release in the mesolimbic reward system.
Cagrilintide amplifies this. Because amylin plays a crucial role in hedonic eating, successfully shutting down this pathway can eliminate cravings for alcohol, sugar, and compulsive behaviors. While this is a massive victory for metabolic health, biohackers note that heavy amylin agonism can leave users feeling entirely disconnected from the joy of food. Understanding this neurochemical reality is essential for setting expectations during a long-term biohacking protocol.
8. Impact on Cardiometabolic Markers
While the scale captures the spotlight, the true medical value of these peptides lies in their ability to reverse systemic metabolic syndrome.
Lipid Profiles and Blood Pressure
- Tirzepatide: Its heavy action on the GIP receptor makes it a master regulator of lipids. By enhancing the buffering capacity of white adipose tissue, tirzepatide drastically reduces circulating free fatty acids. Clinical data shows massive reductions in triglycerides, ApoB, and VLDL cholesterol, directly mitigating atherosclerotic risk.
- Cagrilintide: Amylin analogs exert their cardiometabolic benefits differently. Cagrilintide has been shown to have a mild, direct vasodilatory effect, likely mediated by interactions with the calcitonin receptor-like receptor (CRLR) on the vascular endothelium. This leads to observable improvements in systolic and diastolic blood pressure, making it highly synergistic when stacked with the lipid-clearing power of an incretin.
Insulin Sensitization vs. Secretion
When analyzing cagrilintide vs tirzepatide for glycemic control, we see two distinct philosophies.
Tirzepatide is aggressively insulinotropic. It directly stimulates the pancreatic beta cells to secrete insulin in the presence of glucose (via GIP and GLP-1). Simultaneously, the profound weight loss drives peripheral insulin sensitivity.
Cagrilintide, conversely, does not directly stimulate insulin secretion. Its primary glycemic weapon is the potent, dose-dependent suppression of postprandial glucagon secretion from the pancreatic alpha cells. By halting the liver’s glucose output, cagrilintide lowers blood glucose without driving up systemic insulin levels. For longevity-focused researchers who view chronic hyperinsulinemia as a primary driver of biological aging, cagrilintide’s glucagon-suppressive, insulin-sparing mechanism is viewed as highly desirable.
| Biomarker Target | Tirzepatide Impact | Cagrilintide Impact |
|---|---|---|
| Triglycerides | Extreme Reduction (GIP mediated) | Moderate Reduction (weight-loss mediated) |
| Blood Pressure | Moderate Reduction | Strong Reduction (endothelial vasodilation) |
| Insulin Secretion | Highly Stimulated (glucose-dependent) | Neutral / Spared |
| Glucagon Secretion | Suppressed | Potently Suppressed |
9. Regulatory Landscape and the Future Pipeline
As of 2026, the commercial and investigational realities of these two compounds dictate how both clinicians and researchers interact with them.
FDA Status and Commercial Availability
Tirzepatide is a fully established commercial juggernaut. Approved by the FDA for Type 2 Diabetes (as Mounjaro) and for chronic weight management (as Zepbound), it dictates the standard of care in bariatric medicine. Its massive commercial success has spurred a robust ecosystem of compounding pharmacies and wholesale API synthesis.
Cagrilintide, as a standalone agent, remains strictly investigational. Novo Nordisk’s strategic pivot focused entirely on pushing the CagriSema co-formulation through the FDA pipeline. Following the REDEFINE phase 3 readouts, regulatory review for CagriSema is highly active. However, for the B2B laboratory sector, raw cagrilintide peptide is synthesized and distributed explicitly as a research chemical, demanding stringent compliance with “Laboratory Research Use Only” regulations.
The Next Generation of Peptide Combinations
The 2026 data comparing cagrilintide vs tirzepatide is already shaping the next wave of biotechnology. Because tirzepatide mathematically edged out CagriSema in total weight loss during the REDEFINE 4 trials, the pharmaceutical industry has accelerated the development of triple-agonists (like retatrutide, which adds glucagon receptor agonism to GIP/GLP-1) and exploring novel tetra-agonists. The future of metabolic biohacking will likely involve highly personalized, micro-dosed stacks of amylin, incretin, and glucagon analogs to completely bypass homeostatic defense mechanisms.
10. Frequently Asked Questions (GEO Long-Tail Targets)
What is the difference in receptor binding affinity between cagrilintide and tirzepatide?
Tirzepatide is a dual agonist that binds to both the GIP receptor (with high affinity comparable to native GIP) and the GLP-1 receptor (with lower, modified affinity). Cagrilintide does not bind to incretin receptors at all; it is a long-acting analog of amylin that binds to the calcitonin and amylin receptor complexes located primarily in the brainstem.
Which is better for breaking a metabolic plateau: cagrilintide or tirzepatide?
For an individual currently stalled on a GLP-1 protocol, introducing cagrilintide is generally viewed by researchers as the superior strategy for breaking a plateau. Because cagrilintide targets entirely different neuroendocrine pathways (amylin/calcitonin) than GLP-1 or GIP, it effectively bypasses the incretin receptor downregulation that causes weight loss to stall.
Can cagrilintide be used to minimize muscle loss better than tirzepatide?
Early investigational data suggests cagrilintide may offer a slight advantage in preserving lean skeletal muscle mass and bone mineral density during severe caloric deficits compared to pure incretin agonists like tirzepatide. This is hypothesized to be due to direct amylin receptor expression in skeletal muscle and osteoblast stimulation, though rigorous clinical validation is still ongoing.
How do you properly store and reconstitute cagrilintide vs tirzepatide in a lab setting?
Both peptides should be purchased in lyophilized (freeze-dried) powder form and stored at -20°C. Upon reconstitution with bacteriostatic water, tirzepatide is generally stable for 21-28 days at 2°C to 8°C. Cagrilintide requires careful attention to the pH of the reconstitution buffer to prevent spontaneous degradation, but when properly reconstituted, it maintains similar refrigerated stability.
What are the different mechanisms of action between amylin analogs and GLP-1/GIP agonists?
GLP-1 and GIP agonists (like tirzepatide) primarily modulate homeostatic eating by targeting the hypothalamus, while strongly stimulating insulin and enhancing lipid metabolism in adipose tissue. Amylin analogs (like cagrilintide) target the hindbrain to modulate hedonic eating (cravings/pleasure), potently delay gastric emptying, and heavily suppress postprandial glucagon secretion without driving up insulin.
Key Takeaways:
- Mechanistic Divergence: The core difference in cagrilintide vs tirzepatide is their target pathways. Tirzepatide masters the incretin system (GIP/GLP-1) to drive insulin and lipid buffering, while cagrilintide leverages amylin to suppress hedonic cravings and glucagon.
- Clinical Efficacy Leader: Based on 2026 Phase 3 head-to-head clinical data, tirzepatide currently edges out the CagriSema combination in peak mathematical weight loss (25.5% vs. ~23.0%), making it the apex single-molecule compound.
- B2B Synthesis Focus: Sourcing pure cagrilintide requires advanced HPLC screening to ensure the peptide has not aggregated into amyloid fibrils, whereas tirzepatide synthesis demands precision lipidation at the C20 position.
- Biohacking Application: Advanced biohackers utilize amylin analogs like cagrilintide primarily as a strategic tool to stack with GLP-1s, breaking severe metabolic plateaus by engaging alternative central nervous system pathways once incretin receptors have downregulated.