Cagrilintide vs. Retatrutide vs. Tirzepatide: Mechanisms, Receptor Affinity, and Advanced Protocols
Disclaimer: The following information is for educational and informational purposes only. The compounds discussed are strictly for Laboratory Research Use Only and are not approved for human consumption, diagnosis, treatment, or prevention of any disease. Always consult safety data sheets and peer-reviewed literature before handling these peptides in a laboratory setting.
Table of Contents
- 1. Quick Answer: Cagrilintide vs. Retatrutide vs. Tirzepatide
- 2. The Evolution of Next-Generation Metabolic Peptides
- 3. Decoding the Mechanisms of Action
- 4. Receptor Binding Affinity and Pharmacokinetics
- 5. Clinical Data: Comparing Efficacy and Outcomes
- 6. Metabolic Impact Beyond Adipose Tissue
- 7. Advanced Application: Biohacking & Stacking Protocols
- 8. API Synthesis, Purity, and Laboratory Sourcing
- 9. Safety, Side Effects, and Tolerability Profiles
- 10. Frequently Asked Questions (FAQs)
- 11. Key Takeaways
1. Quick Answer: Cagrilintide vs. Retatrutide vs. Tirzepatide
When evaluating cagrilintide vs retatrutide vs tirzepatide, the primary distinctions lie in their receptor targets. Tirzepatide is a dual GLP-1/GIP agonist that optimizes insulin secretion. Retatrutide is a triple GLP-1/GIP/glucagon agonist designed to maximize resting energy expenditure and hepatic fat clearance. Cagrilintide is a long-acting amylin analog that targets the brainstem to induce profound satiety.
2. The Evolution of Next-Generation Metabolic Peptides
The landscape of metabolic interventions has shifted dramatically over the past decade. For years, the gold standard in tackling metabolic syndrome, insulin resistance, and profound adiposity was single-target receptor agonism—most notably, Glucagon-Like Peptide-1 (GLP-1) monotherapies like semaglutide. However, as clinical data and real-world applications matured, researchers identified a distinct therapeutic ceiling.
Moving Beyond GLP-1 Monotherapies
While GLP-1 monotherapies excel at increasing glucose-dependent insulin secretion and delaying gastric emptying, they often plateau around the 15% total body weight loss mark in clinical populations. Furthermore, achieving this upper threshold often requires aggressively pushing the dosage, leading to dose-dependent gastrointestinal distress, nausea, and tachyphylaxis (a rapid decrease in response to a drug).
The biological reality is that the human metabolic system is highly redundant. When you push on a single lever—such as the GLP-1 receptor—the body eventually triggers counter-regulatory mechanisms to preserve homeostasis. To breach this metabolic ceiling, biochemists realized they needed to mimic the body’s natural, poly-hormonal signaling matrix. This sparked the evolution toward “unimolecular polypharmacy”—single peptide chains designed to bind to multiple distinct metabolic receptors simultaneously.
The Pursuit of Synergistic Efficacy
The transition to dual and triple agonists was not merely about adding overlapping effects; it was about achieving true biological synergy. By combining incretin hormones (GLP-1 and GIP) with glucagon or pairing them with amylin analogs, researchers discovered that these compounds could cross-talk at the cellular level.
For instance, the addition of Gastric Inhibitory Polypeptide (GIP) not only drives superior adipose tissue regulation but also acts as an antiemetic, buffering the intense nausea typically associated with profound GLP-1 receptor activation. This synergy allows for higher functional dosing and deeper metabolic tissue penetration, fundamentally altering how we approach lipolysis, mitochondrial biogenesis, and systemic insulin sensitivity.
3. Decoding the Mechanisms of Action
To truly understand the nuances of these compounds, we must dissect their mechanisms of action at the cellular and systemic levels.
Tirzepatide (The Dual Agonist)
Tirzepatide is an imbalanced dual-incretin receptor agonist. It targets both the GLP-1 and GIP receptors but with a heavy bias toward GIP. When Tirzepatide binds to the GIP receptor on pancreatic beta cells, it drives potent cyclic AMP (cAMP) generation, amplifying glucose-dependent insulin secretion.
However, Tirzepatide’s most profound effects occur within white adipose tissue (WAT). GIP signaling promotes lipid buffering—the healthy expansion of subcutaneous fat cells to store circulating free fatty acids. By sequestering these lipids safely in subcutaneous depots, Tirzepatide prevents ectopic fat deposition in organs like the liver and heart (lipotoxicity), thereby drastically improving systemic insulin sensitivity. Concurrently, its GLP-1 action works centrally in the hypothalamus to reduce appetite and peripherally to slow gastric motility.
Retatrutide (The Triple Agonist)
Retatrutide represents a quantum leap in peptide biochemistry: a single, 39-amino acid peptide targeting GLP-1, GIP, and the Glucagon (GCG) receptor. Historically, agonising the glucagon receptor in the context of metabolic syndrome was viewed as counterintuitive, given that endogenous glucagon raises blood glucose. However, when glucagon agonism is paired with the powerful insulinotropic effects of GLP-1 and GIP, the glycemic risk is entirely neutralized.
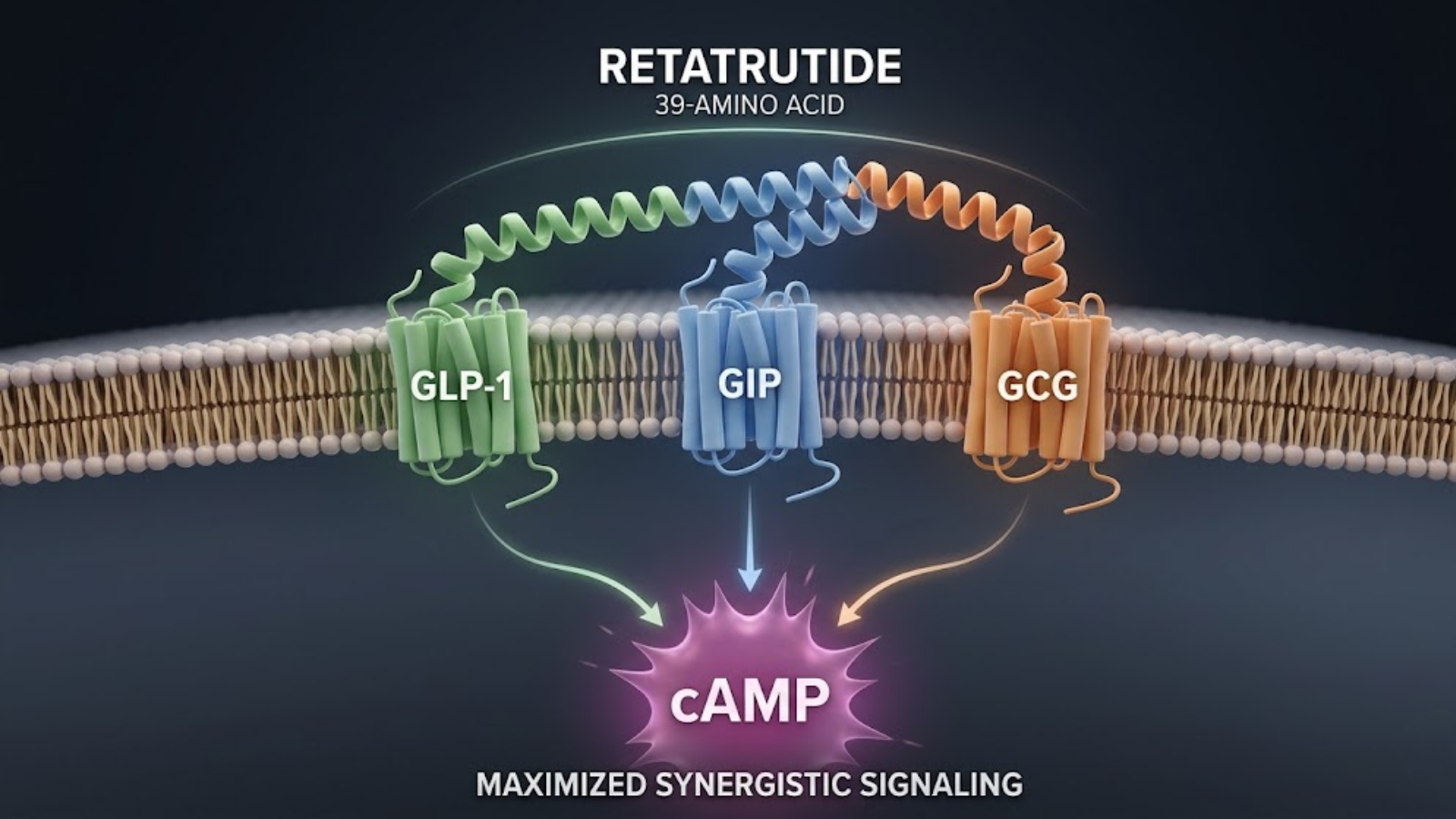
Conceptual Molecular Mechanism: Retatrutide Triple Agonism and cAMP Maximization.
What remains is glucagon’s profound capacity to drive lipolysis and hepatic lipid clearance. Retatrutide signaling at the liver dramatically upregulates beta-oxidation of fatty acids. Furthermore, glucagon receptor activation increases resting energy expenditure (REE) by upregulating thermogenesis in brown adipose tissue (BAT). While Tirzepatide reduces the fuel coming in (appetite suppression), Retatrutide actively turns up the metabolic furnace, increasing the rate at which fuel is burned at baseline.
Cagrilintide (The Amylin Analog)
Unlike Tirzepatide and Retatrutide, Cagrilintide completely bypasses the incretin system. It is a long-acting analog of amylin, a hormone co-secreted with insulin by pancreatic beta cells in response to nutrient intake.
Cagrilintide exerts its primary effects by binding to the amylin and calcitonin receptors located in the area postrema and the nucleus of the solitary tract—regions in the hindbrain (brainstem) that sit outside the blood-brain barrier. Activation of these neural circuits produces an intense, centrally mediated feeling of satiety. Additionally, Cagrilintide profoundly slows gastric emptying and strongly suppresses postprandial glucagon secretion. Because it utilizes an entirely distinct neural and chemical pathway from GLP-1s, it offers an incredible target for combination therapies (such as the experimental CagriSema stack) to overcome incretin tolerance.
4. Receptor Binding Affinity and Pharmacokinetics
For laboratory researchers synthesizing, testing, and handling these peptides, understanding their structural modifications and binding kinetics is critical for designing accurate in-vitro and in-vivo models.
Binding Affinities Compared
The binding affinity of a peptide dictates how effectively it competes with endogenous hormones to activate a receptor. When we examine the analytical profile of cagrilintide vs retatrutide vs tirzepatide, a complex picture emerges:
| Peptide | GLP-1 Receptor Affinity | GIP Receptor Affinity | Glucagon Receptor Affinity | Amylin Receptor Affinity |
|---|---|---|---|---|
| Native Hormones | 100% | 100% | 100% | 100% |
| Tirzepatide | ~18% (Weak) | ~100% (Equipotent) | Null | Null |
| Retatrutide | ~20% (Weak) | ~200% (Super-agonist) | ~40% (Moderate) | Null |
| Cagrilintide | Null | Null | Null | ~100%+ (Highly potent) |
Note: Percentages are relative approximations compared to endogenous native ligands in standard in-vitro bioassays.
Notice that both Tirzepatide and Retatrutide are intentionally designed with “weak” GLP-1 affinity compared to native human GLP-1. This is a deliberate structural engineering choice. By attenuating the GLP-1 signaling, the peptides can be administered at much higher overall milligram doses without triggering debilitating nausea, allowing the GIP and Glucagon actions to achieve maximum systemic saturation.
Half-Lives and Dosing Windows
Achieving a once-weekly dosing profile is the gold standard for metabolic peptides to ensure compliance and steady-state pharmacokinetics.
- Tirzepatide utilizes a C20 fatty diacid moiety attached via a hydrophilic linker, granting it high affinity for serum albumin. This shields the peptide from rapid enzymatic degradation by DPP-4, resulting in a half-life of approximately 5 days.
- Retatrutide also employs a C20 fatty diacid but with strategic amino acid substitutions (like Aib at position 2) to prevent cleavage, yielding a functional half-life of roughly 6 days.
- Cagrilintide achieves stability through structural modifications to the amylin backbone and long-chain fatty acid acylation, pushing its half-life to nearly 7 to 8 days, making it exceptionally stable in circulation.
Molecular Stability
From a laboratory handling perspective, triple agonists like Retatrutide are inherently more complex to synthesize and stabilize than monotherapies. The physical and chemical stability of the lyophilized powder requires strict temperature controls. Aggregation is a notable risk with amylin analogs like Cagrilintide; native amylin is highly amyloidogenic (prone to forming insoluble fibrils). Cagrilintide has been heavily modified with proline substitutions to disrupt this fibril-forming tendency, but stringent laboratory protocols regarding reconstitution pH and temperature must still be maintained.
5. Clinical Data: Comparing Efficacy and Outcomes
The true measure of these molecules is observed in comprehensive clinical trial data. The head-to-head comparison reveals distinct metabolic phenotypes associated with each peptide.
Adipose Tissue Reduction
In the realm of raw fat mass reduction, we are seeing unprecedented numbers.
- Tirzepatide (SURMOUNT Trials): Across 72 weeks of treatment at the maximum 15mg dose, subjects consistently demonstrated an average weight reduction of 20.9% to 22.5%. This shattered the ceiling previously established by semaglutide.
- Retatrutide (TRIUMPH Trials): Phase 2 data showcased an astonishing 24.2% weight reduction at just 48 weeks at the 12mg dose. More critically, the weight loss trajectory showed no signs of plateauing at the 48-week mark, suggesting that the glucagon-driven thermogenesis allows the body to continue burning fat long after incretin-only therapies stall.
- Cagrilintide (Phase 2 & REDEFINE Trials): As a monotherapy, Cagrilintide drives significant weight loss (~10.8%). However, its true clinical power is unleashed when stacked. The CagriSema (Cagrilintide + Semaglutide) phase 2 trials demonstrated a staggering 15.6% weight reduction at only 32 weeks, pointing to massive synergistic potential for multi-pathway targeting.
HbA1c and Glycemic Control
For managing Type 2 Diabetes and severe insulin resistance, Tirzepatide currently reigns supreme. By acting as a robust GIP super-agonist, it restores first-phase insulin secretion remarkably well. In the SURPASS trials, the majority of patients on high-dose Tirzepatide achieved normoglycemic HbA1c levels (<5.7%), effectively putting their diabetes into remission.
Retatrutide also provides excellent glycemic control, though the inherent hyperglycemic pressure of the glucagon agonism requires a delicate balance. The GLP-1 and GIP components successfully overpower the glucagon-induced hepatic glucose output, resulting in a net decrease in HbA1c, but it does not currently outpace Tirzepatide in this specific metric. Cagrilintide is highly effective at flattening postprandial glucose spikes due to its profound delay of gastric emptying, but it lacks the direct insulin-stimulating properties of the incretins.
Visceral Fat and Lean Muscle Retention
One of the most critical challenges in metabolic medicine is ensuring that the weight lost is primarily adipose tissue, not lean skeletal muscle. Severe caloric restriction often leads to sarcopenia.
Tirzepatide has proven highly effective at clearing visceral adipose tissue (VAT)—the dangerous fat surrounding the organs—while improving the ratio of lean mass to fat mass. However, Retatrutide presents a fascinating frontier. Early models suggest that the glucagon receptor agonism, which increases lipid oxidation in the liver, prioritizes the mobilization of stored ectopic and visceral fat as primary fuel substrates. By forcing the body to upregulate thermogenesis via fat oxidation, researchers hypothesize that Retatrutide may offer a superior “quality of weight loss,” protecting skeletal muscle better than profound appetite suppression alone, though long-term Phase 3 body-composition scans are highly anticipated to confirm this mechanism.
6. Metabolic Impact Beyond Adipose Tissue
While subcutaneous fat loss is the most visible metric, the true longevity and healthspan benefits of these peptides occur on a systemic, organ-deep level. Evaluating the cardiometabolic impact of cagrilintide vs retatrutide vs tirzepatide reveals why these molecules are being positioned as broad-spectrum treatments for metabolic dysfunction-associated steatotic liver disease (MASLD) and cardiovascular pathology.

Physiological Targeting Map: Brainstem signaling vs. Hepatic clearance vs. Subcutaneous storage.
Hepatic Steatosis (Fatty Liver)
MASLD, formerly known as NAFLD, is a massive driver of systemic insulin resistance and liver fibrosis. Tirzepatide has shown strong efficacy in reducing liver fat volume, largely secondary to its profound weight loss and GIP-mediated lipid repartitioning. By improving subcutaneous adipose tissue’s capacity to store lipids, Tirzepatide effectively “drains the sink,” preventing ectopic fat from overflowing into the liver.
Retatrutide, however, is a paradigm-shifting compound for hepatic health. Because the liver possesses an extraordinarily high density of glucagon receptors, Retatrutide exerts a direct, localized effect on hepatocytes. In Phase 2 clinical trials, patients taking the 8mg and 12mg doses of Retatrutide experienced relative liver fat reductions of up to 81.4% and 86.0%, respectively, at 24 weeks. Even more astonishingly, in a significant sub-population of the trial, Retatrutide completely resolved hepatic steatosis, returning liver fat to normal, healthy baseline levels in under six months. This is achieved because glucagon signaling directly stimulates hepatic lipolysis (fat breakdown), inhibits de novo lipogenesis (new fat creation), and drives the mitochondrial beta-oxidation of fatty acids.
Cardiovascular Biomarkers
All three compounds positively modulate cardiovascular risk factors, but they do so through slightly different downstream mechanisms.
- Tirzepatide: Drives significant reductions in apolipoprotein B (ApoB), triglycerides, and low-density lipoprotein (LDL) cholesterol. Furthermore, the SURMOUNT trials demonstrated marked reductions in high-sensitivity C-reactive protein (hsCRP), a primary marker of systemic and vascular inflammation.
- Retatrutide: Mirrors the lipid-lowering effects of Tirzepatide but pushes triglyceride clearance even further, likely due to its enhanced hepatic lipid metabolism.
- Cagrilintide: While it also lowers cardiovascular risk via weight reduction, its direct vascular effects are less pronounced than those of the incretins. However, by strictly controlling postprandial glucose excursions and reducing overall metabolic load, it significantly lowers the glycemic damage inflicted on the endothelial lining of blood vessels.
7. Advanced Application: Biohacking & Stacking Protocols
For the advanced B2C biohacker, longevity enthusiast, or self-experimenter, monotherapy is often just the starting point. When subjects push past the 12-to-18-month mark on standard protocols, metabolic adaptation is inevitable.
The core principle of advanced biohacking with metabolic peptides is understanding receptor downregulation and metabolic homeostasis. When you bombard the GLP-1 and GIP receptors with a high-affinity agonist for an extended duration, the body naturally downregulates receptor density and sensitivity to defend its current body mass set point. This is the physiological mechanism behind the dreaded “weight loss plateau.” To breach this, researchers and biohackers are designing synergistic stacks that target unadapted, naive receptor pathways.

Advanced Biohacking Protocol Mapping: Vials, CGM integration, and biometric tracking.
Designing a Synergistic Stack
The most potent example of synergistic stacking currently under clinical investigation is the combination of an incretin (GLP-1/GIP) with an amylin analog (Cagrilintide).
If a subject is adapted to Tirzepatide, their incretin pathways are highly saturated. By introducing Cagrilintide, you engage a completely distinct neurochemical pathway. Cagrilintide binds to calcitonin and amylin receptors in the hindbrain. This induces an immediate, profound sense of early satiation (the feeling of being full after just a few bites of food) that operates independently of the GLP-1 receptor.
| Base Peptide (Primary Action) | Add-on Peptide (Secondary Action) | Target Receptors Engaged | Primary Protocol Goal |
|---|---|---|---|
| Tirzepatide | Cagrilintide | GLP-1, GIP, Amylin, Calcitonin | Extreme appetite suppression, breaking severe metabolic plateaus, mimicking CagriSema. |
| Retatrutide | None (Monotherapy) | GLP-1, GIP, Glucagon | Maximizing energy expenditure (REE) and deep visceral fat clearance. |
| Semaglutide | Retatrutide (Micro-dose) | GLP-1, GIP, Glucagon | Transitioning off GLP-1 monotherapy to introduce lipolytic glucagon effects. |
How to Transition Between Compounds
Transitioning from a dual-agonist like Tirzepatide to a triple-agonist like Retatrutide requires calculated titration. Because Retatrutide introduces glucagon receptor agonism, subjects cannot simply transition milligram-for-milligram without risking sympathetic nervous system overstimulation (tachycardia, anxiety, insomnia).
A standard biohacking protocol for transitioning involves a “washout and bridge” strategy. For example, a subject on 10mg of Tirzepatide weekly might reduce their Tirzepatide dose to 5mg while simultaneously introducing a micro-dose of Retatrutide (e.g., 1mg to 2mg). Over a 4-to-6-week period, the Tirzepatide is systematically titrated down to zero, while the Retatrutide is slowly titrated up. This allows the liver and cardiovascular system to adapt to the new glucagon signaling without shocking the autonomic nervous system.
Breaking the Metabolic Plateau
When navigating the nuances of cagrilintide vs retatrutide vs tirzepatide, Retatrutide is often viewed as the ultimate plateau-breaker. When extreme caloric deficit and GLP-1/GIP agonism fail to yield further fat loss, it is usually because the basal metabolic rate (BMR) has downregulated to match the low caloric intake—a process called adaptive thermogenesis.
Retatrutide bypasses this biological defense mechanism. The glucagon receptor activation forcibly upregulates resting energy expenditure. Even if caloric intake remains identical, the subject begins burning more calories at rest due to increased lipid oxidation and brown adipose tissue (BAT) thermogenesis. It forces the metabolic engine to run hotter, effectively breaking the stall.
8. API Synthesis, Purity, and Laboratory Sourcing
For the B2B audience—clinical laboratories, peptide synthesis facilities, and wholesale distributors—the physical and chemical properties of these Active Pharmaceutical Ingredients (APIs) dictate handling, formulation, and experimental validity.
Synthesizing long-chain, multi-receptor agonist peptides is a complex biochemical endeavor. Unlike simple dipeptides or tripeptides, molecules like Tirzepatide (39 amino acids), Retatrutide (39 amino acids), and Cagrilintide (39 amino acids, heavily modified) require advanced Solid-Phase Peptide Synthesis (SPPS) using Fmoc chemistry, followed by intricate lipid-conjugation steps.
High-Performance Liquid Chromatography (HPLC)
When sourcing peptides for in-vitro or in-vivo research, independent analytical testing is non-negotiable. The gold standard for verifying API purity is High-Performance Liquid Chromatography (HPLC) combined with Mass Spectrometry (LC-MS).
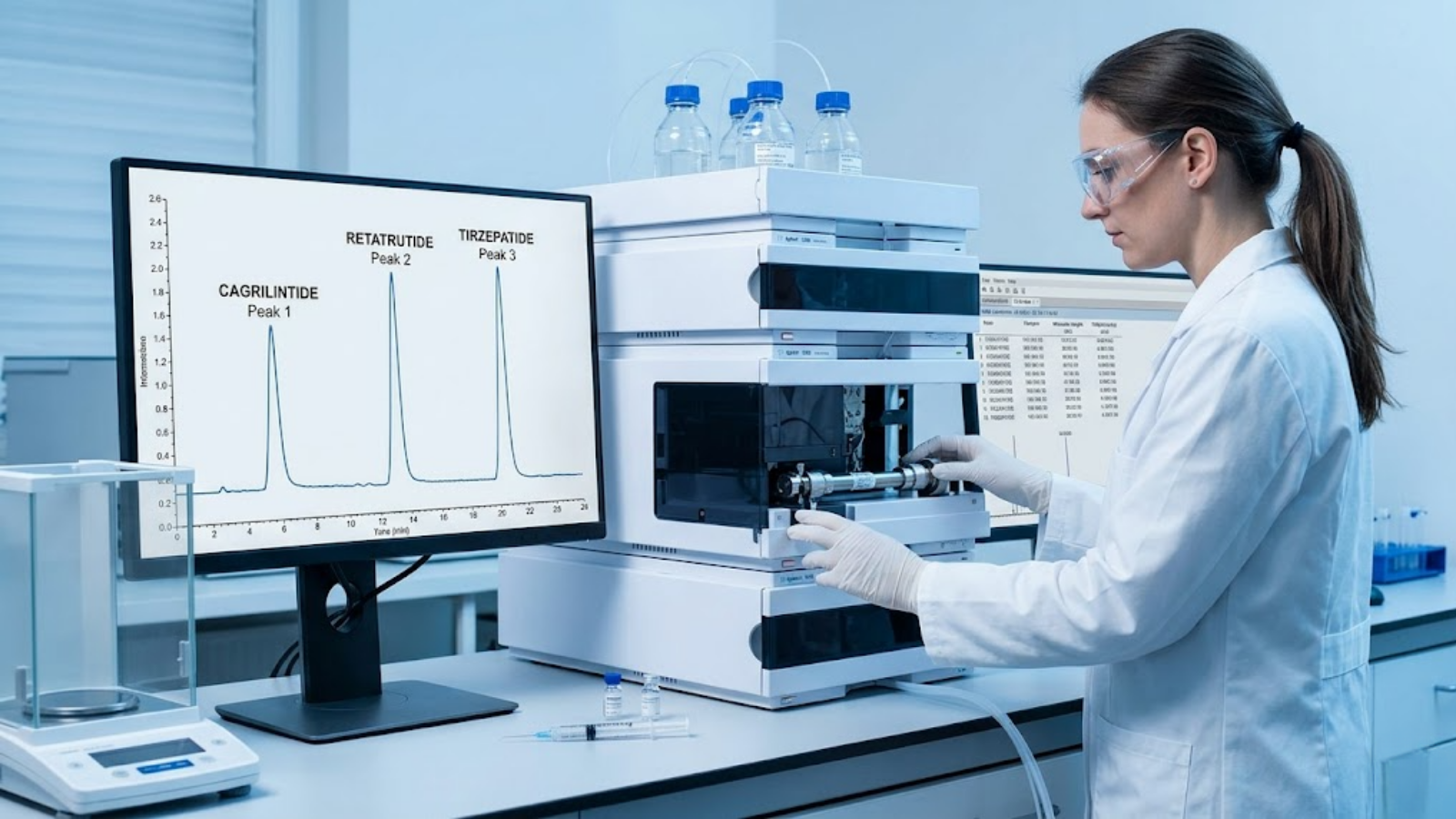
Laboratory validation via HPLC isolating specific compound peaks.
A reliable Certificate of Analysis (COA) must demonstrate a chromatographic peak purity of >99%. For complex lipidated peptides, researchers must specifically look out for:
- Desamido impurities: Where asparagine or glutamine residues have degraded.
- Truncated sequences: Incomplete synthesis chains missing specific amino acids.
- Aggregation: Particularly relevant for Cagrilintide, which, despite structural modifications, still retains some amylin-like propensity to aggregate if exposed to improper pH.
Lyophilization and Reconstitution
Peptides are supplied as lyophilized (freeze-dried) powders. To maintain the structural integrity of the fatty diacid side chains found on Tirzepatide and Retatrutide, the lyophilization process must occur under strict vacuum and ultra-low temperatures.
Another critical B2B concern is the counterion present in the lyophilized powder. Most raw synthesized peptides contain Trifluoroacetic Acid (TFA) salts leftover from the cleavage process. For standard in-vitro receptor binding assays, TFA is generally acceptable. However, for in-vivo animal models, high levels of TFA can be cytotoxic. High-tier synthesis laboratories will perform a salt-exchange process to replace TFA with an acetate or hydrochloride salt, which is vastly safer for biological application.
Sourcing Safely
Wholesale buyers and laboratory managers must rigorously vet suppliers. When acquiring cagrilintide vs retatrutide vs tirzepatide for preclinical research, sourcing red flags include:
- Refusal to provide third-party, USA-based or European-based quantitative HPLC/MS data.
- Lack of specific molecular weight verification matching the exact theoretical mass of the lipidated sequence.
- Inadequate cold-chain shipping protocols for reconstituted solutions. (While lyophilized powder is highly stable at room temperature for weeks, extreme heat during transit can initiate peptide degradation).
9. Safety, Side Effects, and Tolerability Profiles
Modulating the foundational hormones of the human metabolic system comes with distinct physiological consequences. While all three compounds are remarkably effective, their tolerability profiles diverge significantly based on their receptor affinity.
Gastrointestinal Distress
Gastrointestinal adverse events—primarily nausea, vomiting, diarrhea, and constipation—are the most common side effects across all incretin therapies. However, because Tirzepatide and Retatrutide are engineered with a structurally attenuated (weakened) GLP-1 affinity, they are generally better tolerated at high doses than pure GLP-1 monotherapies like semaglutide. The powerful GIP agonism acts as an antiemetic, buffering the nausea pathway in the brain.
Cagrilintide presents a different GI challenge. Because it drastically slows gastric emptying, the risk of profound dyspepsia (indigestion) and theoretical gastroparesis (stomach paralysis) is elevated, particularly if stacked with a GLP-1 agonist. Researchers utilizing Cagrilintide in animal models must monitor feeding behavior closely to ensure complete food impaction does not occur.
Heart Rate and CNS Effects
The most notable safety distinction lies with Retatrutide. Glucagon receptor agonism has a direct chronotropic effect on the heart. In clinical trials, subjects on Retatrutide experienced dose-dependent increases in resting heart rate (RHR), sometimes elevating by 5 to 10 beats per minute.
Furthermore, glucagon can stimulate the sympathetic nervous system, leading to hyperarousal, mild anxiety, or insomnia in sensitive subjects. For this reason, individuals with pre-existing arrhythmias, severe uncontrolled hypertension, or profound cardiovascular disease are often steered toward Tirzepatide, which has a deeply established, highly protective cardiovascular safety profile without the stimulatory glucagon effects.
Titration Protocols
To mitigate these adverse events, absolute adherence to slow titration protocols is mandatory.
- Micro-dosing: Many advanced biohackers attempt to bypass side effects by splitting the weekly dose. Instead of a single 10mg injection of Tirzepatide, they may administer 5mg every 3.5 days. This effectively flattens the pharmacokinetic curve, reducing the sharp peak (Cmax) that triggers nausea while maintaining a higher trough level for sustained efficacy.
- Starting low: With Retatrutide, initiating research protocols at the absolute minimum effective dose (e.g., 1mg to 2mg) and holding that dose for a full four weeks is critical to allow the cardiovascular system to adapt to the new glucagon-mediated chronotropic stress.
10. Frequently Asked Questions (FAQs)
What are the distinct receptor binding affinities of cagrilintide vs retatrutide vs tirzepatide?
Tirzepatide is a dual-agonist targeting GLP-1 (weakly) and GIP (strongly). Retatrutide is a triple-agonist targeting GLP-1, GIP, and Glucagon, providing unmatched energy expenditure. Cagrilintide bypasses incretins entirely; it is a long-acting amylin analog that targets calcitonin and amylin receptors in the brainstem to induce profound, central satiety.
How does the mechanism of action differ when stacking cagrilintide with tirzepatide versus using retatrutide alone?
Stacking Cagrilintide with Tirzepatide combines incretin signaling (insulin regulation, fat partitioning) with powerful amylin signaling (extreme appetite suppression). Using Retatrutide alone provides incretin signaling combined with glucagon agonism, which physically increases resting metabolic rate and drives direct hepatic fat oxidation, rather than just suppressing appetite.
Which is better for visceral fat loss: cagrilintide, retatrutide, or tirzepatide?
While Tirzepatide powerfully reduces visceral fat, Retatrutide is structurally superior for this specific goal. Its glucagon receptor agonism specifically targets ectopic fat and hepatic steatosis, forcing the liver to upregulate beta-oxidation and burn deep visceral fat stores for energy at a rate unmatched by dual-agonists or amylin analogs.
Can I switch from tirzepatide to retatrutide or add cagrilintide to break a weight loss plateau?
Yes. If adapted to Tirzepatide, your GLP-1/GIP receptors are desensitized. Switching to Retatrutide introduces the naive Glucagon receptor to increase metabolic rate. Alternatively, adding Cagrilintide targets the completely naive Amylin receptor to instantly restore profound appetite suppression. Both are highly effective plateau-breaking strategies used in advanced protocols.
What are the best HPLC testing protocols for verifying cagrilintide and retatrutide API purity?
Laboratories should utilize High-Performance Liquid Chromatography (HPLC) coupled with Mass Spectrometry (LC-MS). Testing must verify >99% chromatographic purity, confirm the exact theoretical molecular weight of the lipidated chains, and screen specifically for desamido impurities, truncated peptide sequences, and potentially toxic trifluoroacetic acid (TFA) salt residues.
11. Key Takeaways
The comparative analysis of cagrilintide vs retatrutide vs tirzepatide highlights a rapid maturation in peptide biochemistry, moving from blunt-force receptor activation to highly nuanced, multi-pathway physiological modulation.
- Tirzepatide remains the foundational gold standard for correcting severe insulin resistance, lowering HbA1c, and driving consistent, well-tolerated weight loss through balanced GLP-1 and potent GIP agonism.
- Retatrutide is the ultimate metabolic engine. By integrating the glucagon receptor, it solves the issue of adaptive thermogenesis, actively increasing the body’s resting energy expenditure and demonstrating unprecedented capacity to reverse hepatic steatosis.
- Cagrilintide serves as the ultimate satiation tool and combination agent. Operating outside the incretin system, it provides a distinct, unadapted biological target (the amylin receptor) capable of completely shutting down the biological drive to consume calories, making it a critical asset for breaking deep metabolic plateaus.
Whether approaching these molecules from a clinical B2B synthesis perspective or a B2C biohacking optimization framework, understanding their distinct receptor affinities, half-lives, and synergistic potential is paramount for designing safe, effective, and transformative metabolic protocols. Always prioritize third-party HPLC/MS purity testing, respect the power of slow titration, and recognize that these potent compounds are advanced tools requiring deep biological literacy to deploy safely.