BPC-157 vs. BPC-159: Molecular Differences, FDA Compliance, and Therapeutic Efficacy
BPC-157 vs. BPC-159: Molecular Differences, FDA Compliance, and Therapeutic Efficacy
Table of Contents
- Quick Answer: The Core Difference
- Introduction: The Peptide Shift
- What is BPC-157? The Foundation
- What is BPC-159? The Modern Alternative
- Molecular Differences: Comparative Analysis
- FDA Compliance and Legal Status
- Therapeutic Efficacy: Which Peptide Heals Faster?
- Administration Routes and Bioavailability
- Dosage Protocols for Researchers and Biohackers
- Safety Profiles, Purity, and Side Effects
- Frequently Asked Questions (FAQs)
- Key Takeaways for Your Protocol
Disclaimer: The following information is for educational and laboratory research purposes only. The compounds discussed, including BPC-157 and BPC-159, are not approved by the FDA for human consumption, diagnosis, treatment, or prevention of any disease. Always consult with a licensed medical professional before considering any peptide therapy or advanced biohacking protocol.
Quick Answer: The Core Difference Between BPC-157 and BPC-159
The core difference between BPC-157 and BPC-159 lies in clinical consensus and regulatory status. BPC-157 is an extensively researched, 15-amino-acid synthetic peptide with proven regenerative efficacy in peer-reviewed literature. Conversely, BPC-159 is primarily a commercial nomenclature or structurally modified supplement alternative engineered to navigate recent FDA compounding restrictions on bulk injectable peptides.
Introduction: The Peptide Shift in the Biohacking and Clinical Landscape
For the better part of the last decade, the landscape of regenerative medicine, tissue repair, and advanced biohacking has been dominated by a singular, highly efficacious molecule: BPC-157. From elite athletes recovering from catastrophic tendon tears to clinical researchers exploring novel treatments for inflammatory bowel disease (IBD), this gastric-derived peptide was heralded as a panacea for systemic healing. However, the ecosystem surrounding peptide therapeutics is currently undergoing a massive, highly disruptive shift.
Why the Shift?
This tectonic shift is not driven by new scientific discoveries invalidating older molecules, but rather by an aggressively tightening regulatory framework. Recently, the United States Food and Drug Administration (FDA) made pivotal updates to its Category 2 bulk compounding list. These regulatory changes severely restricted compounding pharmacies from synthesizing, dispensing, and prescribing traditional injectable BPC-157 for human use. Furthermore, the World Anti-Doping Agency (WADA) explicitly banned the use of BPC-157 for competitive athletes.
The immediate result was a vacuum in both the B2B research supply chain and the B2C biohacking market. Laboratories, wholesale distributors, and functional medicine practitioners suddenly found themselves searching for compliant workarounds. Enter BPC-159. The emergence of this heavily marketed alternative has sparked intense debate regarding chemical reality versus legal strategy.
Setting the Stage
To truly understand the ongoing debate of bpc 157 vs bpc 159, we must strip away the marketing jargon and look at these molecules through the lens of strict biochemistry, pharmacokinetics, and regulatory compliance. Are we looking at a legitimate, next-generation peptide sequence with superior bioavailability, or are we witnessing a clever nomenclature pivot designed entirely to bypass FDA import and compounding bans? To answer this, we have to establish the foundational mechanisms of the original molecule before deconstructing its modern counterpart.
What is BPC-157? The Foundation of Gastric Peptide Therapy
Body Protection Compound-157 (BPC-157) is not a naturally occurring compound in the human body in its isolated form; rather, it is a synthetically produced sequence based on a larger protective protein found natively in human gastric juice. To understand its therapeutic efficacy, we must look at its highly specific structural profile and the cellular cascades it initiates upon administration.
Molecular Structure (The Pentadecapeptide)
At its core, BPC-157 is a pentadecapeptide, meaning it consists of an exact sequence of 15 amino acids. The specific sequence is highly conserved: Gly-Glu-Pro-Pro-Pro-Gly-Lys-Pro-Ala-Asp-Asp-Ala-Gly-Leu-Val.
From a biochemical standpoint, this specific sequence is highly stable, particularly when synthesized as an arginine salt (BPC-157 Arginate). The native gastric protein from which it is derived is responsible for protecting the mucosal lining of the stomach from the highly acidic environment (pH 1.5 – 3.5) required for digestion. By isolating this active 15-amino-acid fragment, researchers unlocked a molecule capable of surviving harsh enzymatic degradation while retaining immense cellular signaling capabilities.
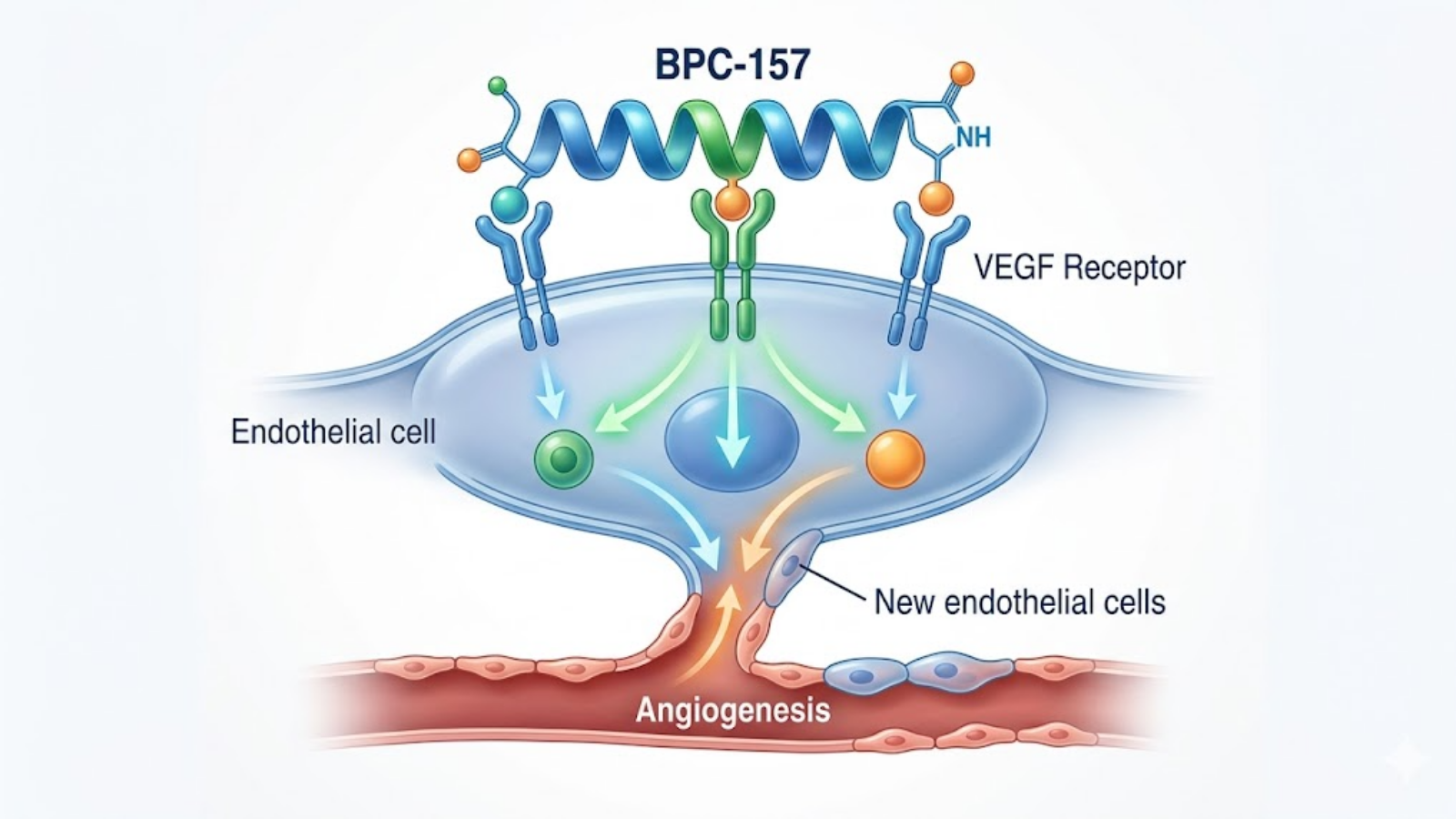
Figure 1: Conceptual visualization of the BPC-157 molecular mechanism stimulating angiogenesis via VEGF upregulation.
Primary Mechanisms of Action
BPC-157 does not act as a traditional hormone or anabolic agent; it operates as a sophisticated signaling molecule that modulates several highly complex biological pathways:
- Angiogenesis via VEGF Upregulation: The most profound mechanism of BPC-157 is its ability to stimulate angiogenesis—the physiological process through which new blood vessels form from pre-existing vessels. BPC-157 achieves this by upregulating the expression of Vascular Endothelial Growth Factor (VEGF) and its receptors. By driving VEGF, the peptide rapidly increases microvascular density at the site of injury, delivering oxygen, fibroblasts, and nutrients crucial for the synthesis of new collagen matrices.
- Nitric Oxide (NO) Pathway Modulation: BPC-157 exerts immense control over the endothelial nitric oxide synthase (eNOS) pathway. Nitric oxide is critical for vasodilation and vascular homeostasis. Interestingly, BPC-157 acts as a modulator rather than a simple agonist; it can protect endothelial cells from both NO depletion (such as in NSAID-induced gastric ulcers) and NO toxicity (overexpression), stabilizing the vascular network during the inflammatory phases of healing.
- FAK-Paxillin and EGR-1 Pathways: On a cellular level, BPC-157 accelerates the migration and proliferation of tendon fibroblasts. It does this by activating the FAK-paxillin (Focal Adhesion Kinase) pathway, which is essentially the cellular machinery responsible for cell motility. Additionally, it stimulates Early Growth Response protein 1 (EGR-1), a transcription factor directly involved in the formation of new collagen and the repair of musculoskeletal tissues.
The Weight of Clinical Data
The scientific literature backing BPC-157 is dense and spans over three decades. In vivo animal models have consistently demonstrated its capacity to completely heal transected Achilles tendons, repair crushed muscle tissue, heal bone fractures by stimulating osteoblast generation, and rapidly close fistulas and gastrointestinal ulcers. While large-scale, phase III human clinical trials are lacking (largely due to the inability to aggressively patent a naturally derived sequence), the sheer volume of peer-reviewed data establishes BPC-157 as a gold-standard benchmark in regenerative biochemistry.
What is BPC-159? Understanding the Modern Alternative
If BPC-157 is the extensively documented gold standard, what exactly is BPC-159? For laboratory researchers, synthesis chemists, and biohackers alike, this is where the waters become chemically and legally murky.
The Chemical Distinction
Unlike BPC-157, which has a universally recognized and immutable 15-amino-acid sequence, “BPC-159” is not universally defined in standard biochemical literature. When analyzing Certificates of Analysis (COAs) and mass spectrometry data from various B2B wholesalers and B2C supplement brands, BPC-159 generally falls into one of three distinct categories:
- A Modified Sequence Derivative: In some cases, chemists will alter one or two amino acids in the sequence or add a specific functional group. The goal is to create an analogue that mimics the receptor affinity of BPC-157 while remaining technically distinct enough to bypass specific patents or FDA bans targeting the exact “157” sequence.
- A Proprietary Complex or Blend: Many BPC-159 products on the commercial market are simply standard BPC-157 (often the arginate salt version) bound to distinct absorption enhancers, such as SNAC (Sodium N-[8-(2-hydroxybenzoyl)amino]caprylate), to dramatically improve oral bioavailability. The “159” label is utilized purely as a branding differentiator for this oral matrix.
- A Strategic Nomenclature Pivot: In the most common scenario, particularly within the dietary supplement space, “BPC-159” is used as a legal shield. Because the FDA has aggressively targeted BPC-157, companies re-label their products to avoid algorithmic flags from payment processors, regulatory agencies, and customs borders.
The “159” Nomenclature and the Dietary Supplement Pivot
The rise of BPC-159 is intrinsically tied to the Dietary Supplement Health and Education Act (DSHEA). Because BPC-157 was historically compounded and injected (a medical procedure), it fell under strict pharmaceutical scrutiny. To keep the therapeutic benefits accessible to the biohacking community, manufacturers pivoted to oral capsules. By utilizing a slightly modified nomenclature—BPC-159—and marketing it strictly for “gut health” or “gastric support” rather than “injury repair,” companies attempt to navigate the highly complex regulatory grey zone of dietary supplements.
Current Literature vs. Commercial Application
This is the most critical distinction for any B2B laboratory researcher or advanced biohacker to understand: there is an overwhelming asymmetry in the scientific literature. If you query PubMed or clinical trial databases for BPC-157, you will yield hundreds of results detailing specific molecular pathways, dosage toxicologies, and tissue-specific healing rates. If you query “BPC-159,” the peer-reviewed data is virtually non-existent. The commercial application of BPC-159 relies entirely on “borrowed science”—the assumption that because it is a structurally similar analogue or derivative of BPC-157, it will inherently possess the exact same regenerative properties. While pharmacologically plausible, it lacks empirical, independent verification.
Molecular Differences: BPC 157 vs BPC 159
To optimize a clinical protocol or formulate a wholesale product, one must understand the practical molecular differences between these two entities, specifically regarding how they survive the human digestive tract and bind to cellular receptors.
Structural Integrity and Gastric Stability
The original BPC-157 acetate salt (the form most commonly found in early injectable research vials) is notoriously unstable in gastric acid. If swallowed, the enzymes in the stomach rapidly cleave the peptide bonds, destroying the 15-amino-acid sequence before it can reach systemic circulation. To combat this, biochemists developed BPC-157 Arginate—binding the peptide to the amino acid arginine. This profoundly increased its structural integrity, allowing it to survive the low pH of the stomach and exert both localized healing in the gut and systemic effects elsewhere.
Formulations marketed as BPC-159 are almost exclusively designed for oral administration. The molecular engineering (whether a true sequence alteration or a proprietary blending technique) is heavily focused on gastric stability. The theoretical advantage of a true BPC-159 analogue is an optimized pharmacokinetic profile that resists enzymatic degradation without the need for complex, highly acidic buffering agents, making it ideal for encapsulated delivery.
Receptor Affinity and Half-life
In biochemistry, even the substitution of a single amino acid can drastically alter a peptide’s three-dimensional folding pattern, thereby changing its receptor binding affinity.
If a BPC-159 formulation utilizes an altered sequence, we must theoretically account for a shift in half-life. Standard BPC-157 acts rapidly; its half-life is relatively short, requiring daily or twice-daily dosing to maintain the continuous upregulation of VEGF and FAK pathways. Some modified BPC-159 analogues are engineered to have a longer biological half-life, theoretically allowing for less frequent oral dosing while maintaining steady-state plasma concentrations. However, without independent pharmacokinetic assays, this remains a theoretical advantage extrapolated from standard peptide engineering principles rather than a proven clinical reality.
Comparative Analysis: Core Properties
To synthesize the complex data for both wholesale compounders and end-user biohackers, the following table breaks down the crucial distinctions driving the bpc 157 vs bpc 159 conversation.
| Property / Metric | BPC-157 (Standard / Arginate) | BPC-159 (Commercial / Analogue) |
|---|---|---|
| Amino Acid Sequence | Standardized 15-AA (Pentadecapeptide) | Variable (Modified analogue, or proprietary blend) |
| Primary Administration | Subcutaneous Injection, Oral (Arginate) | Strictly Oral (Capsules, Sublingual) |
| Gastric Stability | Low (Acetate) / High (Arginate) | Very High (Engineered for digestion resistance) |
| FDA Regulatory Status | Category 2 Bulk Compounding (Restricted) | Grey Market / Marketed as Dietary Supplement |
| Peer-Reviewed Literature | Extensive (Thousands of citations) | Minimal to None (Relies on extrapolated data) |
| Primary Target Audience | B2B Clinical Research, Elite Athletics | B2C Biohackers, Holistic Gut Healing Protocols |
| WADA Status | Banned for in/out of competition use | Subject to umbrella bans on peptide analogues |
FDA Compliance and Legal Status: The Elephant in the Lab
You cannot have a comprehensive discussion regarding bpc 157 vs bpc 159 without addressing the regulatory elephant in the room. For decades, BPC-157 existed in a regulatory grey area—widely utilized by compounding pharmacies, prescribed by functional medicine physicians, and openly discussed in sports medicine. That era has abruptly ended, forcing a rapid evolution in how these peptides are sourced and labeled.
BPC-157 and the FDA Category 2 Bulk Compounding List
In late 2023, the FDA made a definitive ruling regarding the compounding of specific peptide sequences. The agency relegated BPC-157 to the “Category 2” bulk compounding list. In plain English, this means the FDA determined that there is not enough large-scale, phase III human clinical data to support its safety profile, nor does it possess an active Investigational New Drug (IND) application.
Consequently, 503A and 503B compounding pharmacies in the United States are legally prohibited from synthesizing, compounding, and dispensing BPC-157 for human use. This effectively removed the most reliable, sterile, and physician-supervised vector for acquiring the peptide, pushing the demand into the unregulated “research chemical” market.
WADA Regulations and Athletic Bans
Simultaneously, the World Anti-Doping Agency (WADA) took a hardline stance. BPC-157 is explicitly banned for use by athletes both in-competition and out-of-competition. It is classified under “Non-Approved Substances” (S0), as it is not currently approved by any governmental regulatory health authority for human therapeutic use. If you are a tested athlete, BPC-157 will trigger an adverse analytical finding.
How BPC-159 Navigates the Regulatory Framework
This hostile regulatory environment is precisely what birthed the widespread commercialization of BPC-159. By structurally modifying the peptide—or simply marketing a proprietary blend under a novel nomenclature—supplement companies attempt to sidestep the FDA’s specific ban on the “BPC-157” sequence.
Furthermore, by moving away from sterile injectables (which are stringently regulated as medical devices and pharmaceuticals) and pivoting to oral capsules marketed under the Dietary Supplement Health and Education Act (DSHEA), companies classify BPC-159 as a “gastric support” or “gut health” supplement. While this allows advanced biohackers to maintain access to BPC-like therapeutics, it places the burden of verifying purity, safety, and actual chemical composition squarely on the consumer.
Therapeutic Efficacy: Which Peptide Heals Faster?
When assessing the therapeutic efficacy of bpc 157 vs bpc 159, we must draw a firm line between localized tissue repair and systemic mucosal healing. The “better” peptide is entirely dependent on the specific biological target you are trying to regenerate.
Tendon, Ligament, and Musculoskeletal Repair
For acute physical trauma—a torn rotator cuff, a ruptured Achilles tendon, or severe muscle crush injuries—BPC-157 remains the undisputed champion. The literature explicitly demonstrates that injecting BPC-157 near the site of injury accelerates the proliferation of tenocytes (tendon cells) and upregulates the FAK-paxillin pathway, which is essential for collagen network formation. Because injectable BPC-157 bypasses the digestive tract, it achieves peak plasma concentrations rapidly, delivering high-density angiogenic signaling directly to avascular tissues (tissues with poor blood supply, like tendons).
BPC-159, largely limited to oral administration, is theoretically less effective for acute localized trauma. While systemic upregulation of VEGF will eventually reach a damaged tendon, the localized concentration will be significantly lower than a direct subcutaneous injection of 157.
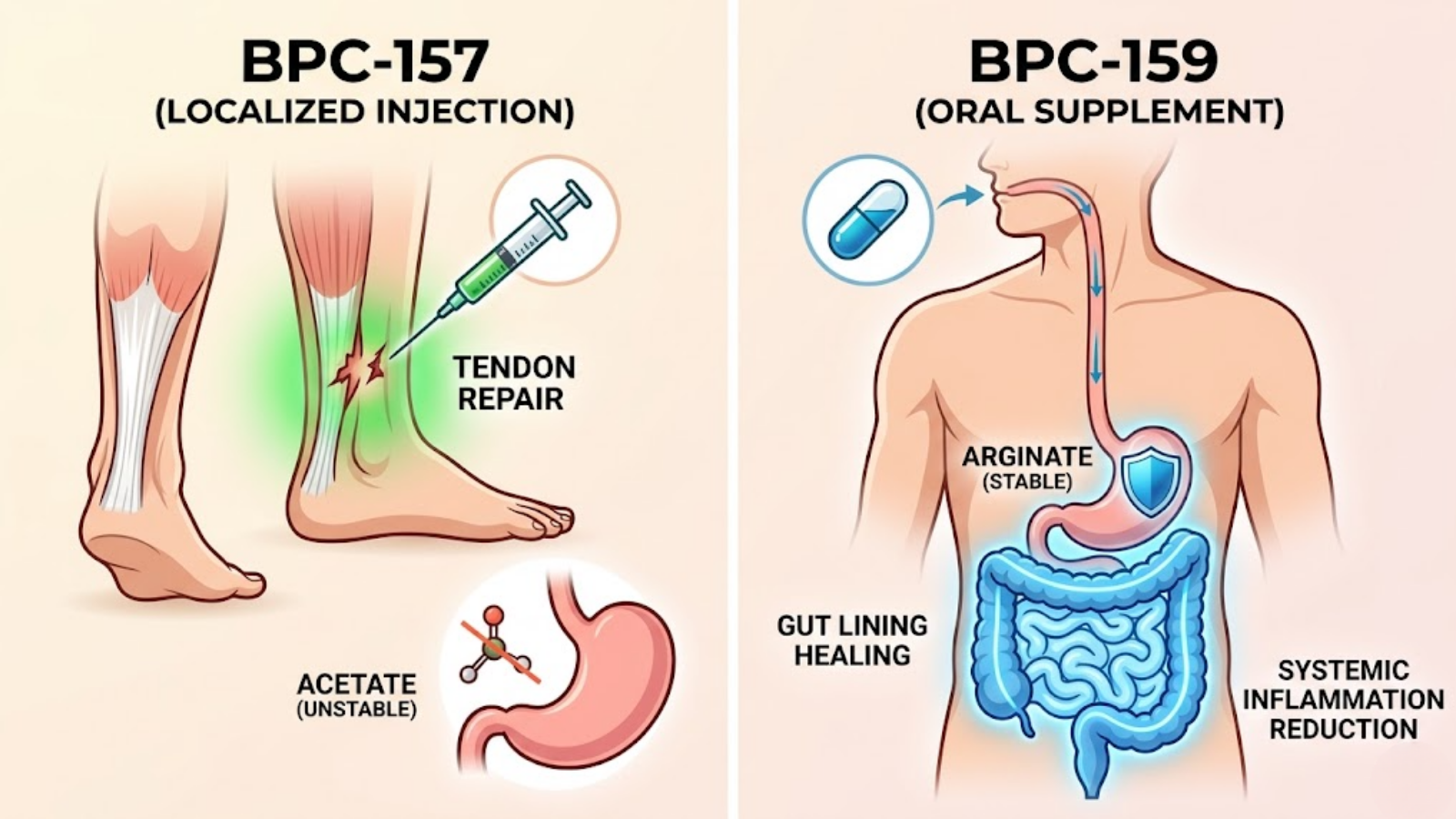
Figure 3: Physiological targeting map contrasting localized tissue repair (BPC-157) vs. systemic GI healing (BPC-159).
Gastrointestinal Healing and Gut Permeability
This is where the paradigm shifts. The native protein that BPC-157 is derived from is inherently designed to heal the gut. For conditions like increased intestinal permeability (Leaky Gut Syndrome), Irritable Bowel Syndrome (IBS), Crohn’s disease, and NSAID-induced gastric ulcers, oral administration is actually preferred.
Because BPC-159 is engineered for extreme gastric stability (often utilizing arginate salts or absorption enhancers), an oral capsule delivers the peptide directly to the inflamed mucosal lining of the stomach and intestines. It interacts directly with the tight junctions of the gut endothelium, downregulating systemic inflammation and physically repairing the cellular barrier. For gut health, oral BPC-159 (or stable oral BPC-157) offers profound, direct-contact healing.
Neurological Recovery and Systemic Inflammation
Emerging research indicates that BPC-157 possesses significant neuroprotective properties. It has been shown to modulate the dopaminergic and serotonergic systems, potentially offering relief from toxin-induced neurological damage, chronic stress, and even alcohol withdrawal. It crosses the blood-brain barrier (BBB) to exert these effects. Assuming a true BPC-159 analogue shares a similar molecular weight and lipophilicity, it theoretically offers the same systemic anti-inflammatory and neuroprotective benefits, though clinical data specific to the “159” sequence in neurological models is currently lacking.
Administration Routes and Bioavailability
The pharmacokinetic reality of any peptide is dictated by its route of administration. Peptides are fragile chains of amino acids; getting them into the bloodstream intact is a monumental biochemical challenge.
Subcutaneous Injections: The Traditional Gold Standard
Historically, researchers and clinicians relied on subcutaneous (Sub-Q) injections for BPC-157. Utilizing a small insulin syringe, the peptide is injected into the fat layer just beneath the skin, ideally adjacent to the site of injury.
- The Advantage: 100% bioavailability. The peptide entirely bypasses first-pass metabolism in the liver and the destructive enzymatic environment of the gastrointestinal tract.
- The Drawback: It requires sterile compounding, bacteriostatic water for reconstitution, strict cold-chain storage, and the psychological hurdle of self-injection.
Oral Capsules: Systemic vs. Localized GI Effects
The BPC-159 market is dominated by oral capsules. To achieve systemic bioavailability, these capsules rely on advanced pharmacology. They must resist the stomach’s low pH (often via the Arginate salt form) and utilize permeation enhancers to slip through the intestinal wall into the bloodstream.
- The Advantage: Ease of use, high compliance, exceptional for treating gut-centric pathology, and currently easier to source legally.
- The Drawback: Decreased systemic bioavailability. Even the most stable oral BPC-159 will suffer some degradation in the gut, meaning you must ingest a higher milligram dose to achieve the same systemic blood concentrations as a microgram injection.
Intranasal and Topical Applications
Some fringe biohacking protocols are exploring intranasal sprays and transdermal creams. Intranasal administration attempts to bypass the blood-brain barrier via the olfactory nerve pathway, theoretically maximizing neurological benefits. Topical creams are utilized for localized joint pain. However, due to the molecular weight of pentadecapeptides, transdermal absorption is incredibly poor without harsh chemical solvents like DMSO, making these routes highly inefficient compared to Sub-Q or oral methods.
Dosage Protocols for Advanced Biohackers and Researchers
Note: The following dosages are aggregated from standard laboratory research models, clinical compounding guidelines, and advanced biohacking literature. They are not medical prescriptions.
Standard Research Dosages for BPC-157
In clinical research, BPC-157 is dosed strictly by body weight, typically in the range of **2.5 to 3.75 micrograms (mcg) per kilogram of body weight**.
- For a 200lb (90kg) researcher: This equates to roughly **250mcg to 350mcg per day**.
- Acute Injury Protocol: For severe trauma, this dose is often split into two administrations (e.g., 250mcg in the morning, 250mcg in the evening) to maintain steady-state plasma levels of the peptide, as its half-life is relatively short (roughly 4 to 6 hours).
Adjusting the Protocol for BPC-159 Supplements
Because BPC-159 is taken orally, the dosage must be adjusted upward to account for the inevitable loss of peptide during digestion and hepatic first-pass metabolism.
- Standard Oral Protocol: High-quality BPC-159 supplements are typically dosed at **500mcg to 1,000mcg (1mg) per day**.
- Timing: For gut healing, oral BPC is best administered on an empty stomach, either first thing in the morning or just before bed, allowing the peptide maximum contact time with the mucosal lining without competing with digestive enzymes breaking down food.
Cycling and Synergistic Stacking (The Wolverine Protocol)
BPC is rarely run indefinitely. A standard research cycle lasts between **4 to 6 weeks**, followed by an equal amount of time off. This prevents receptor downregulation and ensures the body does not become reliant on exogenous angiogenic signaling.
In advanced biohacking circles, BPC is almost always stacked with **TB-500 (Thymosin Beta-4)**. While BPC-157 upregulates angiogenesis and tendon repair, TB-500 regulates cellular actin, radically accelerating cell migration and muscle tissue regeneration. Together, they form a synergistic cascade often referred to colloquially as the “Wolverine Protocol,” capable of halving recovery times for severe musculoskeletal injuries. Researchers interested in this synergy often utilize a pre-mixed BPC-157 TB-500 Combo.
Safety Profiles, Purity, and Potential Side Effects
Peptide therapy is generally considered to have a high safety profile compared to traditional pharmaceuticals or anabolic steroids, largely because these are signaling molecules mimicking native biological processes. However, the unregulated nature of the current market introduces significant risks.
The Crucial Role of HPLC Purity Testing
The primary danger of utilizing BPC-159 or grey-market BPC-157 is not the peptide itself, but the synthesis process. Peptide synthesis is complex; if done poorly, it leaves behind toxic cleavage byproducts, heavy metals, and bacterial endotoxins (TFA salts).
Whether you are a B2B laboratory sourcing wholesale powder or a B2C biohacker buying capsules, you must demand independent, third-party **High-Performance Liquid Chromatography (HPLC)** and **Mass Spectrometry (MS)** reports. A product should test at a minimum of 98% purity. If a vendor cannot provide a verifiable, recent Certificate of Analysis (COA), do not ingest their product.

Figure 2: Professional laboratory setting emphasizing the importance of HPLC purity testing for research peptides.
Known Side Effects
While generally well-tolerated, some researchers report the following side effects:
- Lethargy/Fatigue: Due to its interaction with the central nervous system and modulation of neurotransmitters, some users report feeling unusually tired, particularly in the first week of use.
- Anhedonia: A rare but documented side effect is a temporary flattening of emotions or a decrease in dopamine-driven motivation, likely tied to BPC’s modulatory effect on the dopaminergic system.
- Histamine Reactions: Localized redness, itching, or swelling at the injection site (for subcutaneous routes).
- Gastrointestinal Upset: Ironically, while it heals the gut, the initial introduction of high-dose oral peptides can cause mild nausea or changes in bowel movements.
Long-Term Safety Data and the Angiogenesis Caveat
The most critical safety caveat involves angiogenesis. BPC-157 rapidly creates new blood vessels. If a researcher has an existing, undiagnosed cancer or tumor, creating a highly efficient new blood supply is incredibly dangerous, as tumors require angiogenesis to grow and metastasize. Anyone with a personal or strong family history of cancer should strictly avoid angiogenic peptides. Furthermore, multi-year, longitudinal safety data on humans simply does not exist.
Frequently Asked Questions
Which is better for joint repair: BPC 157 or BPC 159?
Injectable BPC-157 is definitively better for localized joint, tendon, and ligament repair. Subcutaneous administration allows you to deposit the peptide directly adjacent to the avascular tissue, maximizing the concentration of regenerative signaling right where the injury occurred, bypassing the digestive tract entirely.
Does oral BPC-159 have the same effects as injectable BPC-157?
Yes and no. Oral BPC-159 (if properly stabilized) is highly effective for systemic issues, specifically healing the gastrointestinal tract, reducing systemic inflammation, and reversing leaky gut. However, it is significantly less efficient at targeting acute musculoskeletal injuries compared to localized BPC-157 injections due to the loss of bioavailability during digestion.
Will BPC-159 trigger a positive test in WADA-regulated sports?
Yes, it is highly likely. WADA operates on an “umbrella” protocol. While their ban explicitly names BPC-157, it also covers any structurally similar analogues, mimetics, or derivatives. If BPC-159 acts upon the same pathways, it will be considered a doping violation. Do not use either compound if you are a drug-tested competitive athlete.
How does BPC-159 avoid the FDA ban on BPC-157?
BPC-159 navigates the FDA compounding ban by existing outside the pharmaceutical regulatory framework. By altering the nomenclature and packaging it as an oral “dietary supplement” or “gastric support matrix” under DSHEA, companies avoid the strict regulations applied to injectable peptides compounded by 503A pharmacies.
Where can researchers source wholesale BPC safely?
Sourcing must be done through dedicated, US-based research chemical supply houses that publicly post independent, third-party HPLC and Mass Spectrometry testing for every batch. Avoid overseas “white label” suppliers without verifiable COAs, as the risk of heavy metal and endotoxin contamination is unacceptably high.
Key Takeaways: Making the Right Choice for Your Protocol
- The Core Distinction: The bpc 157 vs bpc 159 debate is largely driven by regulatory evasion rather than groundbreaking molecular discovery. BPC-157 is the clinically proven, heavily researched molecule. BPC-159 is generally an oral supplement or analogue designed to bypass recent FDA compounding restrictions.
- Match the Route to the Pathology: If you are trying to heal a torn rotator cuff or Achilles tendon, injectable, localized BPC-157 remains the gold standard. If you are battling IBS, leaky gut, or gastric ulcers, an oral, highly stable BPC-159 capsule is the superior choice.
- Beware of the Literature Gap: Acknowledge that the thousands of peer-reviewed studies detailing miraculous healing mechanisms are explicitly based on the 15-amino-acid BPC-157 sequence. Claims made by BPC-159 products are extrapolated assumptions, not independently verified clinical data.
- Purity is Paramount: The FDA and WADA crackdowns have pushed the supply chain into the grey market. Never administer a peptide—oral or injectable—without first verifying its purity and sterility via independent HPLC and mass spectrometry reports.
- The Synergistic Power: For advanced tissue regeneration, combining BPC (for angiogenesis and vascular repair) with TB-500 (for actin regulation and cellular migration) provides the most comprehensive recovery protocol available in modern biohacking.

Figure 4: Conceptual illustration of an advanced biohacking and medical optimization protocol including peptide analogs.