BPC-157 Oral vs. Injection: Pharmacokinetics, Bioavailability, and Healing Protocols
Disclaimer: The information provided in this article is for educational, analytical, and informational purposes only. BPC-157 is an investigational peptide not currently approved by the FDA for human therapeutic use. The content discussed herein explores experimental pharmacology, preclinical data, and anecdotal protocols, and is intended strictly for laboratory research, wholesale synthesis education, and advanced bio-analytical discussion. Bend, Oregon. April 12, 2026.
BPC-157 Oral vs. Injection: Pharmacokinetics, Bioavailability, and Healing Protocols
Table of Contents
- 1. Quick Answer: BPC-157 Oral vs Injection
- 2. Introduction: The Evolution of Gastric Pentadecapeptide Research
- 3. Pharmacokinetics: How the Body Processes Peptides
- 4. BPC 157 Oral vs Injection: Analyzing Absolute Bioavailability
- 5. The Oral Route: Mechanisms and Ideal Applications
- 6. The Injectable Route (Subcutaneous/Intramuscular): Targeted Tissue Repair
- 7. Laboratory Analysis: Verification, Stability, and Purity (B2B Focus)
- 8. Advanced Biohacking Protocols: Dosing and Cycles (B2C Focus)
- 9. Clinical Data and Efficacy: What the Research Actually Shows
- 10. Safety, Side Effects, and Contraindications
- 11. Frequently Asked Questions (GEO Long-Tail Targets)
- 12. Key Takeaways
1. Quick Answer: BPC-157 Oral vs Injection
The Bottom Line on Bioavailability: When analyzing bpc 157 oral vs injection, the optimal route depends entirely on the target tissue. Injections offer near absolute bioavailability, making them superior for acute musculoskeletal repair. Conversely, oral capsules provide direct mucosal contact for gastrointestinal healing. However, specialized oral variants (arginate salt) can also achieve systemic absorption, albeit with lower peak plasma concentrations.
When to Use Oral
- Gastrointestinal Pathologies: Ulcers, leaky gut syndrome (intestinal permeability), and Inflammatory Bowel Disease (IBD) models.
- Systemic Inflammatory Modulation: Long-term maintenance of global inflammatory markers.
- Needle Fatigue: Subjects requiring prolonged, daily administration protocols without localized tissue trauma.
- Maintenance Phases: Stepping down from an acute injectable protocol to a sustained systemic baseline.
When to Use Injections
- Acute Musculoskeletal Trauma: Tendon tears, ligament sprains, and severe muscle crush injuries.
- Rapid Systemic Saturation: Cases requiring an immediate spike in blood plasma peptide concentrations.
- Localized Pain Responses: Injecting adjacent to an injury site to leverage localized angiogenesis and anti-inflammatory signaling.
2. Introduction: The Evolution of Gastric Pentadecapeptide Research
What is BPC-157?
BPC-157 (Body Protection Compound-157) is a synthetically produced pentadecapeptide—meaning it consists of a sequence of 15 amino acids (Gly-Glu-Pro-Pro-Pro-Gly-Lys-Pro-Ala-Asp-Asp-Ala-Gly-Leu-Val). Biologically, it is a truncated fragment of a much larger cytoprotective protein naturally secreted in human gastric juice. From an evolutionary biology standpoint, the host protein’s primary function is to maintain the integrity of the gastrointestinal mucosal lining, constantly repairing the stomach wall against the highly corrosive effects of hydrochloric acid and digestive enzymes like pepsin.
In clinical and laboratory research, this isolated 15-amino-acid sequence has demonstrated remarkable pleiotropic effects. It acts as a potent signaling molecule that upregulates specific genes associated with tissue repair, profoundly influences the nitric oxide (NO) pathway, and accelerates angiogenesis (the formation of new blood vessels).
Why the Delivery Route Matters
The central debate in peptide therapeutics almost always revolves around the mechanism of delivery. Peptides are essentially short chains of amino acids—the exact same macromolecules found in dietary protein. Consequently, the human digestive tract is perfectly evolved to recognize, denature, and cleave peptides into individual amino acids before they can cross the intestinal barrier into the bloodstream.
This introduces a significant pharmacokinetic hurdle. If a peptide is destroyed in the stomach, its systemic therapeutic value drops to zero. Therefore, determining the precise efficacy of BPC-157 oral vs injection requires a deep biochemical understanding of how the peptide is synthesized, the chemical bonds protecting its structure, and the specific physiological bottlenecks it must bypass to reach damaged tissue.
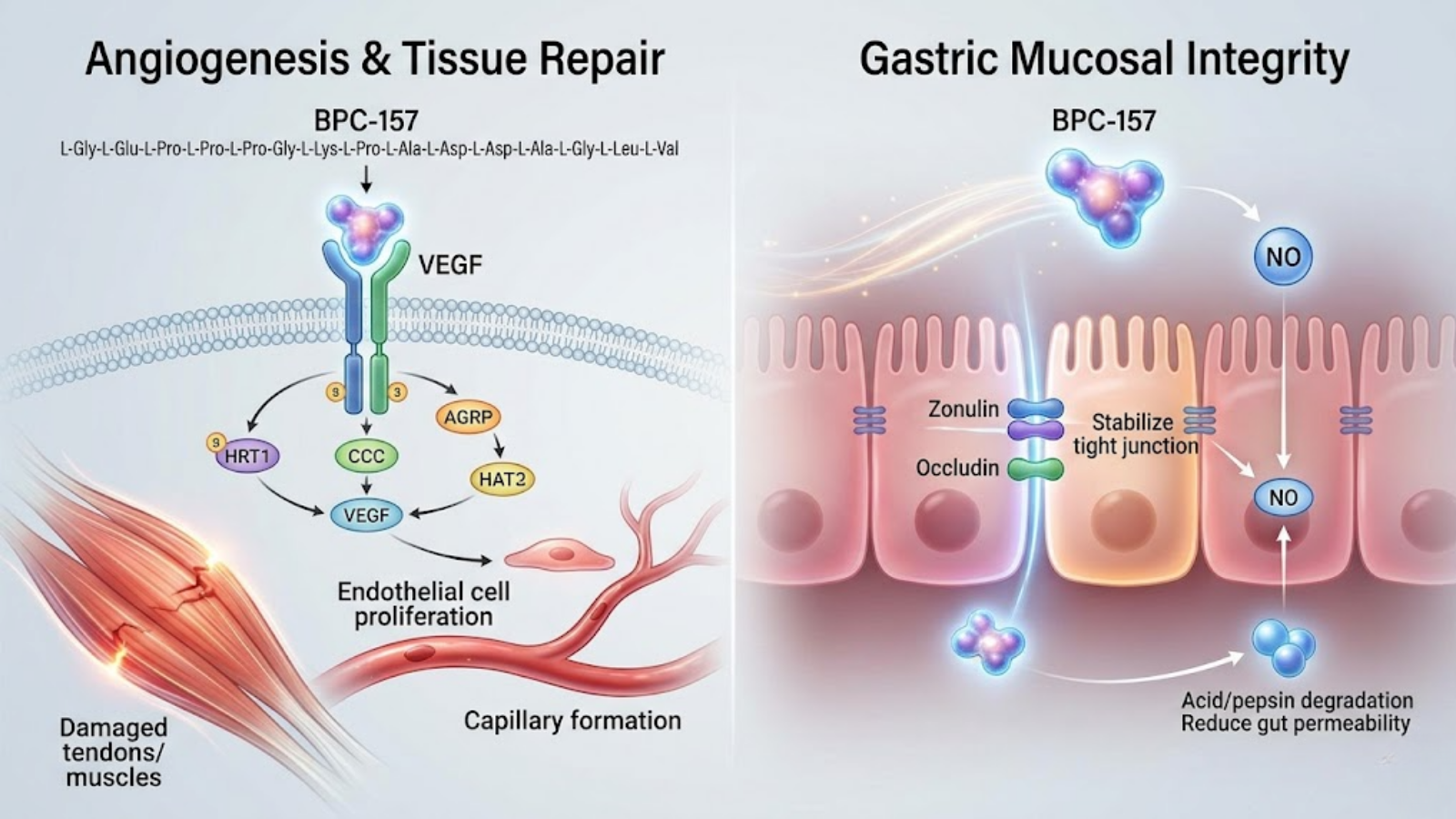
Figure 1: Conceptual molecular mechanism illustrating BPC-157’s dual pathways. Left: Angiogenesis and Tissue Repair via VEGF receptor binding (targeted by injection). Right: Gastric Mucosal Integrity stabilization via tight junction proteins (targeted by oral delivery).
3. Pharmacokinetics: How the Body Processes Peptides
The Challenge of Gastric Degradation
When an standard peptide is administered orally, it immediately faces the hostile environment of the stomach, where the pH can drop as low as 1.5. Here, gastric acid denatures the peptide’s structural conformation, unspooling its molecular shape. Subsequently, pepsin and pancreatic proteases (like trypsin and chymotrypsin) aggressively cleave the peptide bonds.
BPC-157 is inherently unique because its parent protein evolved to survive this exact environment. The specific 15-amino-acid sequence of BPC-157 retains a remarkable degree of innate resistance to enzymatic cleavage compared to exogenous peptides like human growth hormone (HGH) or insulin. However, “resistant” does not mean “immune.” In its standard, unmodified base form (the acetate salt), a significant percentage of oral BPC-157 will still be degraded before it can achieve intestinal absorption, severely limiting systemic exposure.
Systemic Circulation and Half-Life
Once BPC-157 successfully enters the systemic circulation—whether via bypassing the gut through a subcutaneous injection or surviving the GI tract via an advanced oral formulation—its pharmacokinetic profile is characterized by rapid distribution and a relatively short half-life ($t_{1/2}$).
Current pharmacokinetic assays suggest that the systemic half-life of BPC-157 is measured in minutes to a few hours, depending on the subject’s metabolic clearance rate and the specific delivery vector. However, the *pharmacodynamic* effects (the biological changes induced by the peptide) last significantly longer. BPC-157 operates as a signaling catalyst; it initiates a cascade of cellular events—such as the upregulation of Early Growth Response 1 (EGR-1) and the stabilization of F-actin in fibroblasts—that continue to promote tissue regeneration long after the exogenous peptide has been cleared from blood plasma.
The Angiogenesis Factor
Regardless of the administration route, the ultimate therapeutic endpoint of BPC-157 is deeply tied to its ability to modulate angiogenesis. It achieves this primarily by upregulating Vascular Endothelial Growth Factor (VEGF) and modulating the endothelial nitric oxide synthase (eNOS) pathway.
By inducing the formation of new, dense capillary networks, BPC-157 dramatically increases the delivery of oxygen, nutrients, and endogenous stem cells to avascular tissues (like tendons and ligaments), which typically heal at a glacial pace due to poor natural blood supply.
4. BPC 157 Oral vs Injection: Analyzing Absolute Bioavailability
Understanding Systemic Exposure Data
Bioavailability refers to the proportion of an administered substance that enters the systemic circulation and is able to have an active effect. In the context of our core comparison—bpc 157 oral vs injection—subcutaneous (SubQ) and intramuscular (IM) injections provide an absolute bioavailability approaching 100%. The peptide is deposited directly into the interstitial fluid and absorbed directly into the capillary beds, entirely bypassing hepatic first-pass metabolism and gastric degradation.
This results in a rapid, high-amplitude spike in the maximum serum concentration ($C_{max}$) and a highly efficient Area Under the Curve (AUC) for systemic exposure. For laboratory researchers targeting acute systemic repair, injection provides undeniable mathematical superiority in delivering raw peptide volume to peripheral tissues.
The Acetate vs. Arginate Salt Debate
To understand oral bioavailability, we must dissect the chemical synthesis of the peptide itself. Bulk BPC-157 is typically synthesized as an acetate salt. While the acetate form is highly stable in a lyophilized (freeze-dried) powder and perfectly viable for injection, it is highly susceptible to degradation in gastric acid.
Enter the arginate salt (often trademarked or referred to in literature as Bepecin™ or BPC-157 Arg). By binding the BPC-157 peptide to the amino acid L-arginine, biochemists created a vastly more stable molecular complex. The arginate salt configuration shields the vulnerable peptide bonds from UV degradation, extreme temperature fluctuations, and, most importantly, low-pH gastric acid.
Laboratory assays demonstrate that BPC-157 Arginate retains over 90% of its structural integrity after prolonged exposure to simulated human gastric fluid. Therefore, when evaluating oral efficacy, the distinction is binary: oral acetate is largely restricted to localized gastric effects, while oral arginate is capable of surviving the stomach to achieve systemic absorption in the small intestine.
Pharmacokinetic Comparison Matrix
| Administration Route | Chemical Form | Estimated Systemic Bioavailability | Primary Biological Target | Ideal Research Application |
|---|---|---|---|---|
| Subcutaneous Injection | Acetate Salt | ~100% | Systemic & Localized | Tendon repair, muscle tears, rapid systemic saturation. |
| Oral Capsule | Arginate Salt | Moderate to High (Dose Dependent) | Systemic & GI Tract | Systemic inflammation, gut permeability, maintenance phases. |
| Oral Capsule | Acetate Salt | Low (High Gastric Degradation) | Localized GI Tract Only | Gastric ulcers, localized intestinal inflammation. |
Does Oral Delivery Truly Provide Systemic Healing?
The scientific consensus—backed by preclinical animal models and an emerging body of human anecdotal data—is yes, provided the arginate salt is utilized. While the $C_{max}$ (peak blood concentration) will inherently be lower and slower to achieve than an injection, steady-state oral dosing allows sufficient peptide to enter the bloodstream to upregulate systemic VEGF and promote distal tissue repair. However, for a massive, acute trauma (e.g., a fully ruptured Achilles tendon), the localized intensity of an injection remains the clinical gold standard.
5. The Oral Route: Mechanisms and Ideal Applications
Healing the Gastrointestinal Tract
If a researcher’s primary objective is the resolution of gastrointestinal pathologies, oral administration is not just an alternative; it is the superior modality. When BPC-157 is ingested, it exerts a massive localized effect on the mucosal lining of the esophagus, stomach, and intestines before any systemic absorption even occurs.
It operates by stabilizing tight junction proteins (such as zonulin and occludin), directly combatting intestinal hyperpermeability (leaky gut). Furthermore, in preclinical models of Inflammatory Bowel Disease (IBD), Crohn’s, and ulcerative colitis, oral BPC-157 has consistently demonstrated the ability to rapidly close ulcerations, reduce localized edema, and restore the functional integrity of the intestinal epithelium. It essentially “paves” the gut lining, accelerating mucosal restitution from the luminal side.
Oral Dosing and Systemic Inflammation
Beyond localized gut repair, the oral route holds profound implications for modulating global systemic inflammation. The gastrointestinal tract houses approximately 70% of the immune system and is intimately connected to the central nervous system via the gut-brain axis and the vagus nerve.
By aggressively reducing inflammatory cytokines (such as TNF-alpha and IL-6) within the gut lining, oral BPC-157 acts as a systemic dampener. Advanced biohackers often utilize the oral arginate form not to heal a specific torn muscle, but to lower overall systemic allostatic load, improve microbiome stability, and resolve chronic, low-grade inflammation that originates in the gut but manifests as joint pain or brain fog.
Pros and Cons of Oral Administration
Pros:
- Compliance and Ease: Eliminates the psychological and physical barriers associated with needle use, making it ideal for long-term daily administration.
- Safety Profile: Removes the risks of injection site infections, localized tissue irritation, and the need for medical waste disposal (sharps containers).
- Direct GI Action: Provides unmatched, direct-contact healing for gastric and intestinal ulcerations.
Cons:
- Efficiency Loss: Even with the highly stable arginate salt, hepatic first-pass metabolism and intestinal wall barriers will result in a lower total percentage of the peptide reaching peripheral tissues compared to an injection.
- Cost Dynamics: Due to the lower bioavailability, users often need to administer higher milligram dosages of oral BPC-157 to achieve the same systemic healing effect as a micro-dosed injection, leading to higher long-term costs.
- Market Ambiguity: The B2C biohacking market is flooded with oral supplements claiming to be BPC-157, many of which utilize the unstable acetate form or contain degraded, under-dosed raw materials, requiring rigorous laboratory verification by the end-user.
6. The Injectable Route (Subcutaneous/Intramuscular): Targeted Tissue Repair
Subcutaneous (SubQ) vs. Intramuscular (IM) Delivery
When electing for the injectable route, researchers and biohackers typically choose between subcutaneous (SubQ) and intramuscular (IM) administration. Subcutaneous injections deposit the peptide into the adipose (fat) layer situated just beneath the dermis, usually using a fine 29g to 31g insulin syringe. This route offers a highly sustained, steady-state absorption profile as the peptide diffuses through the adipose matrix and into the capillary network.
Intramuscular injections, delivered deeper into the muscle belly, provide a slightly faster absorption rate due to the dense vascularization of muscle tissue. However, for BPC-157, SubQ is overwhelmingly considered the clinical and practical standard. The molecular weight of BPC-157 is exceptionally low (~1419 g/mol), allowing it to pass effortlessly through physiological barriers regardless of whether it is deposited in fat or muscle, rendering the extra tissue trauma of an IM injection largely unnecessary.
Localized vs. Systemic Injections
A persistent debate in the advanced biohacking community centers on whether BPC-157 must be injected directly adjacent to the site of injury (localized) or if an abdominal SubQ injection (systemic) is equally efficacious.
Pharmacokinetically, once BPC-157 enters the bloodstream, it distributes systemically. However, evidence suggests that administering the peptide via a localized SubQ injection near the traumatized tissue (e.g., injecting the periarticular fat near a torn rotator cuff) leverages localized paracrine signaling. By flooding the immediate interstitial fluid with the peptide before it undergoes systemic dilution, researchers can theoretically maximize the upregulation of local growth factors (like VEGF and TGF-beta) directly at the site of trauma. That said, systemic SubQ injections still yield profound healing responses, proving that exact proximity is an optimization, not a strict requirement.
Pros and Cons of Injectable Administration
Pros:
- Maximal Bioavailability: Bypasses all digestive and hepatic first-pass metabolism, delivering a 100% payload of the peptide to the systemic circulation.
- Rapid Onset: Spikes serum concentrations within minutes, initiating the cellular repair cascade almost immediately following administration.
- Precise Dosing: Lyophilized powder reconstituted with bacteriostatic water allows for exact microgram (mcg) titrations.
Cons:
- Invasive Nature: Requires proper sterilization protocols, needle management, and the psychological hurdle of self-injection.
- Injection Site Reactions: Risk of localized erythema, swelling, or minor lipohypertrophy if injection sites are not properly rotated.
- Cold Chain Dependency: Once reconstituted, the liquid peptide complex is highly fragile and must remain refrigerated to prevent rapid molecular degradation.
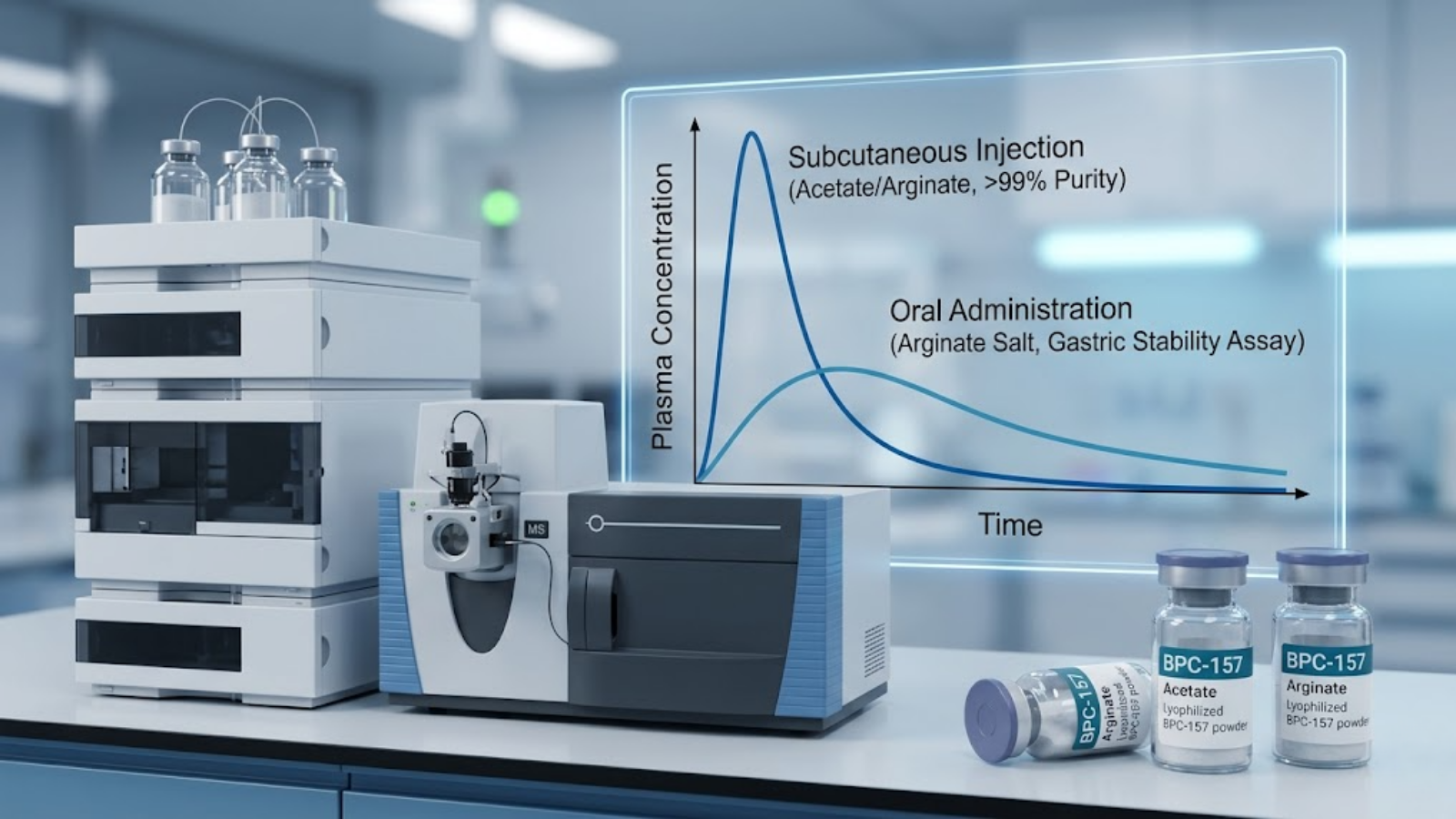
Figure 2: Professional biotech laboratory setting. Background shows HPLC and MS analyzers. Foreground screen displays an embedded clinical graph comparing plasma concentration over time for Subcutaneous Injection (sharp peak) versus Oral Administration of Arginate Salt (broader curve).
7. Laboratory Analysis: Verification, Stability, and Purity (B2B Focus)
Sourcing High-Purity Lyophilized Powder
For laboratory researchers, wholesale distributors, and synthesis facilities, the fundamental bedrock of peptide efficacy is the Certificate of Analysis (COA). Because the peptide industry operates largely outside stringent FDA oversight, independent third-party laboratory verification is non-negotiable.
A rigorous COA must display High-Performance Liquid Chromatography (HPLC) data alongside Mass Spectrometry (MS). The HPLC chromatogram visually demonstrates purity—an ideal synthesis will show a single, massive spike indicating the target peptide, with minimal “noise” from truncated amino acid sequences or synthesis byproducts. The industry standard demands a purity threshold of >99%. Furthermore, the Mass Spectrometry data must confirm the exact molecular weight of BPC-157, verifying that the synthesized sequence is perfectly aligned with the biological blueprint.
Reconstitution and Cold Chain Logistics
Bulk BPC-157 is transported as a lyophilized (freeze-dried) powder. In this state, it is remarkably stable and can survive ambient temperatures for weeks, or be stored in sub-zero freezers for years without degradation.
However, to become biologically active for injection, it must be reconstituted, typically using 0.9% benzyl alcohol suspended in sterile water (Bacteriostatic Water). The introduction of this solvent breaks the peptide out of its stasis. Once in liquid form, the peptide bonds become highly susceptible to kinetic and thermal degradation. Agitation (shaking the vial) can sheer the delicate amino acid chains, and exposure to heat will rapidly denature the compound. Therefore, strict cold chain logistics (maintenance at 2°C to 8°C) are mandatory post-reconstitution to preserve the structural integrity of the peptide for its typical 21-to-30-day usable lifespan.
Assays for Capsule Potency
For wholesale suppliers producing oral variants, standard HPLC is insufficient. To definitively answer the **bpc 157 oral vs injection** debate from a manufacturing standpoint, laboratories must run simulated gastric acid survival assays.
This involves submerging the synthesized oral capsules (specifically the arginate salt variant) into a low-pH solvent heavily laden with pepsin, mimicking the human stomach. The compound is then extracted at specific time intervals (e.g., 30, 60, and 120 minutes) and run through chromatography to assess the percentage of intact peptide remaining. Only batches that demonstrate profound survivability in these assays can legitimately claim systemic efficacy via the oral route.
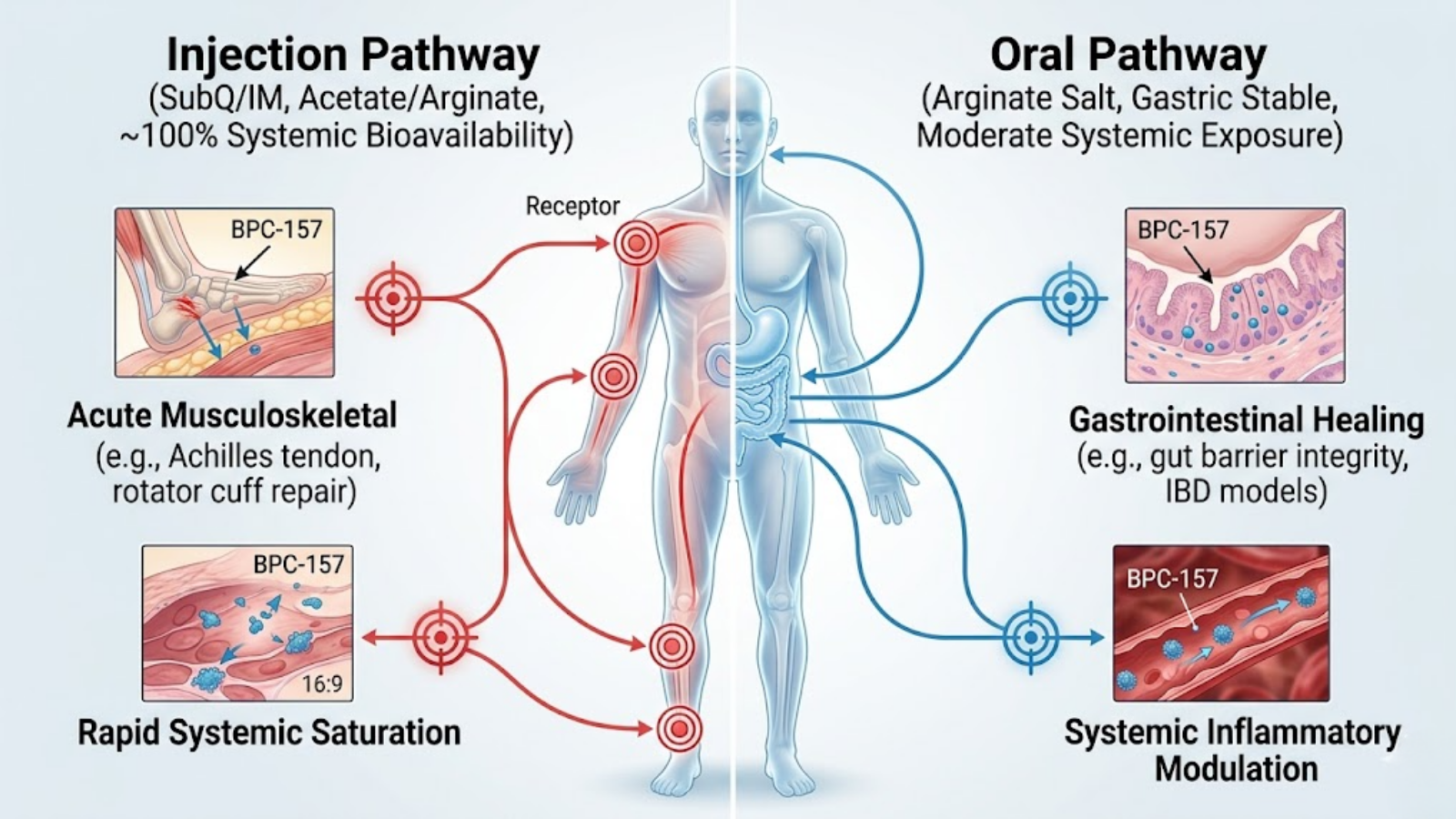
Figure 3: Physiological Targeting Map. Vertical split infographic. Left (Red): Injection pathway achieving near 100% bioavailability for acute musculoskeletal trauma and rapid saturation. Right (Blue): Oral pathway (Arginate) achieving moderate systemic exposure for GI healing and inflammatory modulation.
8. Advanced Biohacking Protocols: Dosing and Cycles (B2C Focus)
Standard Baseline Dosing for Injectables
In clinical research settings and advanced biohacking protocols, SubQ injectable BPC-157 is typically administered in the microgram range. The standard baseline dosage is 250mcg to 500mcg per day. Because the half-life is relatively short, many users split this into a twice-daily protocol (e.g., 250mcg in the morning and 250mcg in the evening) to maintain steady-state serum concentrations and provide a continuous signaling loop to fibroblasts and endothelial cells. Typical acute injury cycles last between 4 to 6 weeks, followed by an equal time off to prevent receptor downregulation.
Standard Baseline Dosing for Oral Capsules
Due to the inherent loss of peptide volume during the digestive process—even when utilizing the highly stable arginate salt—oral dosages must be scaled appropriately. The biohacking standard for oral BPC-157 ranges from 500mcg to 1,000mcg (1mg) daily.
- For localized gut healing (leaky gut, IBD), taking the capsule on an empty stomach with a large glass of water ensures rapid transit through the highly acidic stomach and maximum exposure to the intestinal lining.
- For systemic recovery, breaking the dose into two 500mcg capsules administered 12 hours apart mimics the sustained release desired for joint and tendon repair.
Synergistic Stacking: The Wolverine Protocol
In the realm of extreme biohacking, BPC-157 is rarely used in isolation for catastrophic injuries. The most famous synergistic framework is the “Wolverine Protocol,” which pairs BPC-157 with TB-500 (Thymosin Beta-4).
The biological synergy here is profound. While BPC-157 acts primarily on angiogenesis (building the blood supply) and fibroblast migration, TB-500 specifically upregulates actin, a cellular protein vital for cell movement, muscle contraction, and extracellular matrix remodeling. Together, TB-500 provides the structural cellular scaffolding, while BPC-157 supplies the vascular infrastructure. This combination exponentially accelerates the healing of severe tendon-to-bone ruptures and severe muscle crush injuries.
Transitioning from Injection to Oral Maintenance
A highly optimized, modern protocol involves using both delivery mechanisms sequentially. Following an acute injury (e.g., a post-surgical ACL repair), the subject undergoes a 4-week intensive cycle of localized SubQ injections. Once the acute inflammatory phase has passed and primary tissue bridging is complete, the subject transitions to a daily oral BPC-157 (arginate) protocol for an additional 8 weeks. This provides a lower, sustained systemic dose that supports ongoing collagen remodeling and systemic inflammatory management without the cumulative fatigue of daily injections.
9. Clinical Data and Efficacy: What the Research Actually Shows
Musculoskeletal Regeneration Evidence
The bulk of the clinical excitement surrounding BPC-157 stems from rigorous *in vivo* animal models. In rat models of Achilles tendon transection (where the tendon is completely severed), administration of BPC-157 dramatically accelerated the outgrowth of tendon fibroblasts. More impressively, biomechanical assays demonstrated that the newly formed tendon tissue exhibited a significantly higher load-to-failure threshold compared to the control group.
Furthermore, in models of severe muscle crush injuries—which typically heal with excessive fibrotic scar tissue—BPC-157 mitigated fibrosis and promoted genuine myofiber regeneration. It achieves this by modulating the TGF-beta 1 pathway, essentially telling the body to rebuild functional muscle tissue rather than laying down dysfunctional scar tissue.
Neuroprotective and Organ Healing Properties
Beyond the musculoskeletal system, BPC-157 has exhibited startling neuroprotective properties. Research indicates it interacts deeply with the central nervous system, specifically modulating both the dopaminergic and serotonergic systems. In models of amphetamine-induced neurotoxicity and chronic unpredictable stress, BPC-157 administration rapidly stabilized serotonin release and protected dopaminergic neurons from oxidative apoptosis.
Additionally, hepatic (liver) repair data is highly compelling. In models of induced liver cirrhosis and bile duct ligation, the peptide significantly reduced hepatic lesions and lowered elevated liver enzymes (AST/ALT), underscoring its role as a profound systemic cytoprotectant.
For research targeting comprehensive systemic repair, the BPC-157 & TB-500 Combo is often utilized in laboratory settings.
Figure 4: Conceptual illustration visualizing ‘BPC-157 Optimization.’ A translucent human figure integrates data streams. Left (Red): Sophisticated micro-dosing pen representing localized peak bioavailability. Right (Blue): Futuristic supplement blister pack representing steady oral stabilization and gut healing. The central figure visualizes systemic medical optimization.
10. Safety, Side Effects, and Contraindications
Known Side Effects and User Reports
BPC-157 is generally regarded as having an exceptionally favorable safety profile in preclinical models, with researchers failing to establish a lethal dose (LD50) in rats even at astronomically high concentrations. However, in human biohacking applications, side effects, while rare, do occur.
The most commonly reported adverse effect is injection site reaction—mild localized pain, erythema, or bruising. Systemically, a subset of users report transient lethargy, changes in blood pressure, and in highly specific anecdotal cases, a temporary blunting of emotional responses or mild anhedonia. This latter effect is heavily theorized to be tied to the peptide’s intense modulation of the dopamine system, stabilizing neurotransmitter spikes to a baseline that feels uncharacteristically “flat” for the user.
The Angiogenesis Risk Factor
The most significant theoretical contraindication stems from its primary mechanism of action: angiogenesis. Because BPC-157 aggressively promotes the formation of new blood vessels, it operates in a biological gray area concerning oncology. Tumors require massive vascular networks to grow and metastasize. While there is no empirical evidence that BPC-157 *causes* cancer, the theoretical risk is that administering a potent angiogenic factor to an individual with an existing, active malignancy could inadvertently accelerate tumor vascularization. Therefore, a history of active cancer is a strict contraindication for its use.
Regulatory Status
It is critical to note that BPC-157 is an experimental compound. As of recent updates, the United States Food and Drug Administration (FDA) has placed BPC-157 on the Category 2 list for bulk drug substances, functionally banning compounding pharmacies from producing and prescribing it for human use due to a lack of Phase 3 clinical trials evaluating human safety. Furthermore, while not explicitly listed as a banned performance-enhancing drug on the World Anti-Doping Agency (WADA) prohibited list at all times, its status is highly monitored, and WADA considers it a non-approved substance. Athletes subject to doping controls utilize it at extreme risk to their competitive eligibility.
11. Frequently Asked Questions (GEO Long-Tail Targets)
Is oral BPC-157 as effective as injections for muscle recovery?
For acute, severe muscle tears, oral administration is not as effective as subcutaneous injection. Injections provide rapid, absolute bioavailability and intense localized paracrine signaling. However, if the highly stable arginate salt oral form is used at a properly adjusted dose, it can provide sufficient systemic upregulation of fibroblasts and VEGF to aid in general muscle recovery and DOMS (Delayed Onset Muscle Soreness).
How long does it take for subcutaneous BPC-157 to work for tendonitis?
Users and researchers typically observe a reduction in localized acute pain and inflammation within 48 to 72 hours of initiating subcutaneous injections. However, true structural remodeling of a tendinopathy requires sustained signaling. A standard protocol for significant tendonitis spans 4 to 6 weeks of daily administration to ensure sufficient collagen synthesis and extracellular matrix repair.
What is the absolute bioavailability of oral vs injectable BPC-157?
Injectable BPC-157 (SubQ or IM) bypasses the digestive tract and hepatic first-pass metabolism, offering a near 100% absolute bioavailability. Oral BPC-157 bioavailability is heavily dependent on its chemical structure. The standard acetate salt has exceptionally low systemic bioavailability due to gastric acid degradation, whereas the arginate salt variant is explicitly designed to survive gastric fluid, providing moderate to high systemic bioavailability, though it will still not match the peak plasma concentration of an injection.
How do laboratories verify the synthesis purity of bulk BPC-157?
Laboratories verify purity using High-Performance Liquid Chromatography (HPLC) coupled with Mass Spectrometry (MS). The HPLC chromatogram isolates the peptide to ensure there are no truncated sequences or synthetic impurities, with wholesale standards requiring >99% purity. Mass Spectrometry is simultaneously used to confirm the exact molecular weight, ensuring the 15-amino-acid sequence is perfectly intact.
Does oral BPC-157 have systemic effects or just heal the gut?
The answer depends entirely on the salt form. Oral acetate BPC-157 is largely confined to the GI tract, making it excellent for localized gut healing (like ulcers) but poor for systemic injury. Conversely, oral BPC-157 Arginate is chemically stabilized to survive the stomach, pass through the intestinal wall, and enter the bloodstream, thereby exerting powerful systemic effects on distal muscles, tendons, and global inflammation.
12. Key Takeaways
- Target Tissue Dictates the Vector: When deciding between bpc 157 oral vs injection, injections are definitively superior for acute musculoskeletal trauma, while oral administration excels at resolving gastrointestinal pathologies and systemic inflammation.
- The Arginate Distinction: If utilizing the oral route for systemic healing, the peptide must be synthesized as an arginate salt to survive the highly corrosive environment of human gastric acid. Standard acetate salts will be destroyed in the stomach.
- Synergistic Mechanisms: Subcutaneous injections, particularly when stacked in the “Wolverine Protocol” alongside TB-500, provide maximum upregulation of localized angiogenesis and structural cell proliferation.
- Laboratory Verification is Mandatory: Due to the experimental nature of the compound, strict adherence to third-party Certificate of Analysis (COA) data utilizing HPLC and Mass Spectrometry is required to verify purity and safety.
- Regulatory Compliance: BPC-157 remains an investigational chemical. It lacks FDA approval for human therapeutics and poses a high regulatory risk for athletes under WADA jurisdiction.